The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore what happens when you pass a kidney stone — visualizing calcium oxalate crystal nucleation and growth, stone migration through the urinary tract, ureteral smooth muscle spasm mechanics, and the complete physiological journey from renal pelvis to bladder. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Happens When You Pass a Kidney Stone? (The Atomic Answer)
What happens when you pass a kidney stone is one of the most precisely documented pain experiences in medicine — a predictable sequence of crystal migration, mechanical obstruction, and neurological alarm that has been described as among the most intense sensations the human body can produce.
- The Formation: Kidney stones begin as microscopic crystal nuclei in supersaturated urine — typically calcium oxalate (80% of stones) — that grow over weeks to months into macroscopic stones ranging from 1mm to 10mm+ in diameter.
- The Migration: When a stone enters the ureter — the 3–4mm wide tube connecting the kidney to the bladder — it triggers violent ureteral peristaltic spasms attempting to push the stone downward. This spasm, not the stone itself, is the primary source of the excruciating colic pain.
- The Journey: The stone must travel approximately 25–30cm through the ureter — shown encountering three anatomical narrowings where obstruction is most likely: the ureteropelvic junction (UPJ), the point where the ureter crosses the iliac vessels, and the ureterovesical junction (UVJ).
- The Resolution: Stones smaller than 4mm pass spontaneously in approximately 80% of cases. Stones 4–6mm pass in approximately 60% of cases. Stones larger than 6mm typically require medical intervention.

My 3D Discovery: Rendering the “Crystal That Becomes a Crisis”
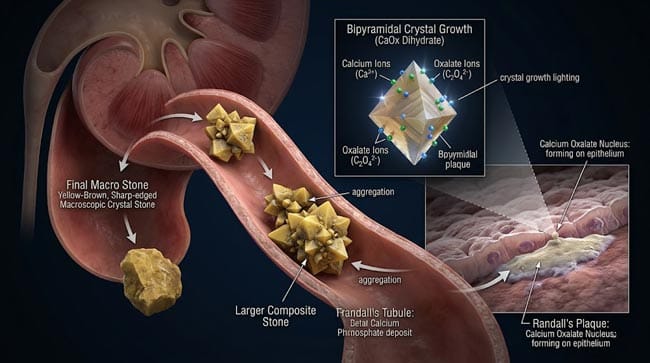
When I was building the kidney stone formation model for this simulation, the most visually striking sequence was the nucleation and growth process. A single microscopic calcium oxalate crystal shown forming in the collecting tubule of a nephron — its geometric molecular structure shown as a precisely ordered lattice of calcium, oxalate, and water molecules.
In the 3D viewport, this crystal shown growing over weeks — each day shown adding new layers of calcium oxalate to its surface, shown as the crystal growing from submicroscopic to millimeter scale in slow, inevitable progression. The crystal’s characteristic bipyramidal geometry shown becoming apparent — the sharp crystalline edges that will later cause the characteristic “peeing glass” sensation during passage.
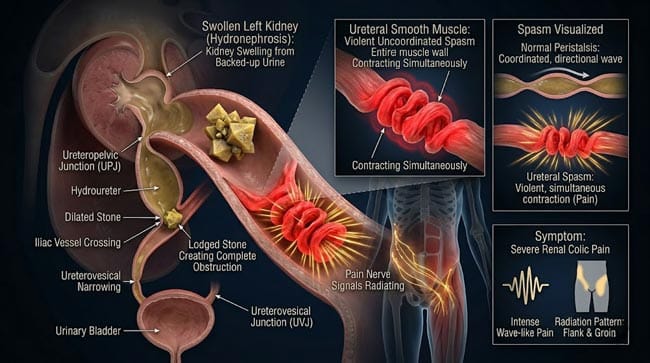
3D Observation: The most medically significant visualization in this simulation is the ureteral spasm sequence. When the stone enters the ureter, I showed the ureteral smooth muscle in real time — the normal peristaltic waves shown as organized, rhythmic contractions traveling smoothly from kidney to bladder. The moment the stone shown arriving at the ureteral lumen, the smooth muscle shown going into violent, uncoordinated spasm — shown as the muscle contracting at full force from multiple directions simultaneously, attempting to push the stone down while also contracting around it. The pressure shown building in the blocked ureter above — shown transmitted back to the renal pelvis and the kidney’s collecting system. This hydronephrotic pressure and the ureteral spasm together shown producing the renal colic that patients describe as the worst pain of their lives.
Stage 1: Kidney Stone Formation — The Crystal Chemistry
The Four Main Stone Types:
In our 3D stone classification model, I rendered the four major kidney stone types:
Calcium Oxalate (80% of all stones) Shown as yellow-brown bipyramidal or monohydrate plaque-shaped crystals. The most common stone type — forms when urine is supersaturated with calcium and oxalate ions. Two subtypes:
- Calcium oxalate monohydrate (whewellite) — shown as dense, dark, harder crystals — more resistant to fragmentation
- Calcium oxalate dihydrate (weddellite) — shown as lighter, more porous crystals — easier to fragment with lithotripsy
Calcium Phosphate (5–10%) Shown as flat, plate-like crystals — associated with high urine pH and certain metabolic conditions including renal tubular acidosis.
Uric Acid (5–10%) Shown as smooth, rounded, radiolucent (invisible on X-ray) stones — the only major stone type that can be dissolved with medication (urine alkalinization). Associated with gout, high purine diet, and metabolic syndrome.
Struvite (5–10%) Shown as large, irregular “staghorn” calculi — formed only in the presence of urease-producing bacteria (Proteus, Klebsiella). Associated with recurrent urinary tract infections.
The Formation Process — Calcium Oxalate:
In our 3D nucleation model, I rendered the complete crystal formation sequence:
Step 1 — Supersaturation: Normal urine contains calcium and oxalate ions at concentrations that keep them in solution. When urine becomes supersaturated — from dehydration (reduced urine volume concentrating all solutes), high calcium excretion (hypercalciuria), high oxalate excretion (hyperoxaluria), or low citrate (a natural crystal inhibitor) — the solution reaches the thermodynamic threshold for crystal nucleation.
Step 2 — Nucleation: A crystal nucleus shown forming at a surface — typically the renal tubular epithelium or an existing Randall’s plaque (subepithelial calcium phosphate deposit shown as a common nucleation site). The nucleus shown as just a few dozen calcium oxalate molecule units — invisible to any imaging but the beginning of the eventual stone.
Step 3 — Crystal Growth: Additional calcium and oxalate ions shown attaching to the nucleus surface — the crystal shown growing layer by layer. Growth rate shown dependent on urine supersaturation — in severely concentrated urine, shown growing millimeters per week; in adequately diluted urine, growth shown essentially stopping.
Step 4 — Aggregation: Multiple smaller crystals shown aggregating together — shown as individual crystal units clustering and fusing into larger composite stones. This aggregation shown dramatically accelerating macroscopic stone development compared to single-crystal growth alone.
Step 5 — Stone Detachment: When the stone grows large enough to detach from the renal papilla — shown as the fragile attachment shown breaking, releasing the stone into the renal pelvis and collecting system.
| Stone Type | Crystal Structure | Color | Main Risk Factors | Medical Dissolution |
|---|---|---|---|---|
| Calcium oxalate | Bipyramidal/plaque | Yellow-brown | Dehydration, high oxalate diet | ❌ Not dissolvable |
| Calcium phosphate | Plate-like | White-gray | High urine pH, RTA | ❌ Not dissolvable |
| Uric acid | Smooth, rounded | Yellow-orange | Gout, low urine pH, high purine diet | ✅ Alkalinization works |
| Struvite | Irregular, staghorn | Gray-white | UTI with urease bacteria | ❌ Requires surgery/antibiotics |
According to the National Kidney Foundation, approximately 1 in 10 people will develop a kidney stone during their lifetime — with recurrence rates of approximately 50% within 10 years without preventive measures. The lifetime risk has been increasing in correlation with rising rates of obesity, diabetes, and dietary changes. NKF: Kidney Stones
Stage 2: The Migration — Journey Through the Ureter
The Ureter Anatomy:
The ureter is a muscular tube connecting the renal pelvis to the bladder — approximately 25–30cm long and only 3–4mm in internal diameter at its narrowest points. In our 3D ureteral model:
- Lumen: Shown as a narrow tube — the internal space through which urine (and stones) must pass
- Urothelial lining: Shown as transitional epithelium capable of stretching
- Smooth muscle layers: Three layers shown (inner longitudinal, outer circular, outer longitudinal) — responsible for peristaltic propulsion
- Adventitia: Outer connective tissue containing blood vessels, lymphatics, and nerve supply
The Three Anatomical Narrowings — Where Stones Get Stuck:
In our 3D anatomical model, I showed the three locations where ureteral diameter is most restricted:
1. Ureteropelvic Junction (UPJ) — where the renal pelvis narrows into the ureter. Internal diameter shown as approximately 2mm at this point — the tightest segment. Stones shown most commonly obstructing here.
2. Crossing of Iliac Vessels — where the ureter crosses over the external iliac artery and vein. The vessel pulsation shown creating a natural pressure point that can impede stone passage.
3. Ureterovesical Junction (UVJ) — where the ureter enters the bladder wall. Shown as a valve-like structure that normally prevents urine reflux — creating a second narrow segment of approximately 1–2mm.
The Migration Mechanics:
When a stone detaches and enters the ureter, two simultaneous events shown occurring:
Normal peristalsis attempts propulsion: The ureter’s smooth muscle shown trying to push the stone downward using its normal peristaltic wave mechanism. However, the stone — unlike fluid urine — shown creating resistance that the normal peristaltic force cannot easily overcome.
Spasm response: The stone’s presence shown triggering an abnormal smooth muscle response — the ureter shown going into violent, uncoordinated spasm. This spasm shown several times more forceful than normal peristalsis — shown as the entire ureteral muscle wall shown contracting simultaneously and repeatedly.
The pressure buildup: Above the obstructed stone, urine shown unable to drain. The renal pelvis shown distending — hydronephrosis shown developing. The intrarenal pressure shown rising — shown transmitted throughout the collecting system. This pressure shown stimulating the dense pain fiber network around the renal capsule.
Stone Passage Timeline by Size:
| Stone Size | Spontaneous Passage Rate | Average Time to Pass | Medical Intervention Needed |
|---|---|---|---|
| <4mm | ~80% | 1–2 weeks | Rarely |
| 4–6mm | ~60% | 2–4 weeks | Sometimes |
| 6–9mm | ~20% | Weeks to months | Usually |
| >9mm | ~5% | Unlikely without intervention | Almost always |
Stage 3: Medical Management — From Alpha-Blockers to Lithotripsy
Conservative Management (for stones <6mm):
Hydration: Shown as the primary treatment — increased fluid intake shown increasing urine flow rate, which shown helping flush the stone through the ureter and reducing urine supersaturation to prevent further growth.
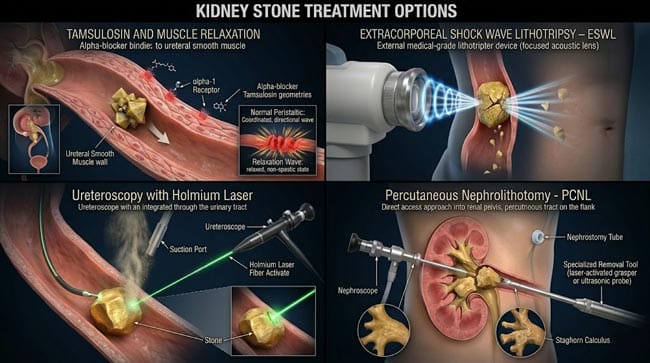
Alpha-blockers (Tamsulosin): The most evidence-based medical intervention for facilitating stone passage. In our 3D pharmacological model, tamsulosin shown blocking alpha-1 adrenergic receptors in the ureteral smooth muscle — shown relaxing the muscle tone and reducing the violent spasm that obstructs passage. Clinical trials shown demonstrating tamsulosin increases spontaneous passage rates by 29–44% for ureteral stones.
Pain management: NSAIDs (ibuprofen, ketorolac) shown as particularly effective for renal colic — they shown reducing prostaglandin production in the ureteral tissue, which shown decreasing both pain signaling and ureteral spasm. Opioids shown providing additional pain relief for severe colic.
Interventional Management:
Extracorporeal Shock Wave Lithotripsy (ESWL): In our 3D lithotripsy model, I showed focused shock waves shown being generated outside the body and focused on the stone using ultrasound imaging guidance. The shock wave shown creating a rapid pressure differential at the stone’s surface — shown causing mechanical fragmentation into smaller pieces that can pass spontaneously.
Ureteroscopy with Laser Lithotripsy: A thin ureteroscope shown being advanced up the urethra, through the bladder, and up the ureter to the stone. A holmium laser fiber shown delivering precise laser energy to the stone — shown fragmenting it into dust or small passable fragments. Shown as the most effective treatment with a stone-free rate exceeding 90%.
Percutaneous Nephrolithotomy (PCNL): For very large stones (>2cm) or staghorn calculi — shown as a direct access to the kidney created through the back — a nephroscope shown being inserted to fragment and remove stone material directly from the collecting system.
FAQ: What Happens When You Pass a Kidney Stone?
Q1: What does passing a kidney stone actually feel like? Renal colic is typically described as the most severe pain many patients have ever experienced — surpassing surgical incision pain, fractures, and in surveys, even childbirth for many respondents. The pain shown coming in waves — coinciding with ureteral spasm contractions. Between spasms, the pain may reduce to a severe ache. The location shifts as the stone moves: flank pain (at the kidney level), then lower abdominal and groin pain (as the stone descends the ureter), then bladder pressure and urinary urgency (as the stone approaches the UVJ). The moment the stone enters the bladder, shown as the severe colic stopping almost immediately — replaced by bladder irritation symptoms.
Q2: What causes some people to form kidney stones and others not to? Multiple genetic and dietary factors determine stone risk. Familial hypercalciuria — genetically elevated urinary calcium — shown as present in approximately 50% of calcium stone formers. Chronic dehydration shown as the most modifiable risk factor — reduced urine volume shown concentrating all solutes above crystallization threshold. High dietary oxalate (spinach, nuts, chocolate) combined with low calcium intake shown increasing oxalate availability for absorption. Low dietary calcium paradoxically increases stone risk — shown as intestinal calcium normally binding oxalate and preventing its absorption. Adequate dietary calcium shown reducing oxalate absorption and urinary excretion.
Q3: Does drinking water really prevent kidney stones? Yes — consistently and significantly. Sufficient hydration shown maintaining urine output above 2 liters per day — shown as keeping solute concentrations below the crystallization threshold. Studies show that increasing fluid intake to produce >2L of urine daily reduces kidney stone recurrence by 50–60%. Specifically shown: lemon juice (citric acid content) shown increasing urinary citrate — a natural crystal inhibitor. Stone prevention shown primarily achieved through diet and hydration rather than medication for most stone formers.
Q4: Can you feel a kidney stone before it starts moving? Most kidney stones are completely silent during their formation period — shown as growing in the renal calyx without causing any symptoms because they do not obstruct urine flow. Many stones shown discovered incidentally on imaging performed for other reasons. Symptoms only develop when the stone enters the ureter and begins obstructing urine flow — the transition from silent to symptomatic shown as often sudden and dramatic.
Q5: After passing a kidney stone, how long before it could happen again? Without preventive measures, the recurrence rate is approximately 50% within 5 years and 70–80% within 10 years for calcium oxalate stones. The recurrence risk shown being highest in the year following the first stone — reflecting the same underlying metabolic conditions that produced the first stone. Dietary modifications (increased hydration, reduced sodium and animal protein, adequate calcium intake) shown reducing recurrence risk by 40–50%. Pharmacological prevention (thiazide diuretics for hypercalciuria, potassium citrate for low urinary citrate, allopurinol for uric acid stones) shown further reducing risk in high-risk individuals.
Conclusion: The Most Precisely Located Pain in Medicine
Kidney stone pain is one of the most diagnostically specific pain syndromes in medicine — its location, character, and migration pattern shown reflecting the stone’s precise position in the urinary tract with extraordinary accuracy. A physician can often determine whether a stone is at the UPJ, mid-ureter, or UVJ simply from the patient’s pain distribution.
In 3D, rendering the complete journey — from crystal nucleation in the collecting tubule through stone growth, detachment, ureteral entry, spasm cascade, and eventual bladder entry — makes the full scope of what the body experiences during kidney stone passage visually immediate.
The stone is the trigger. The ureter’s desperate, spasming attempt to pass it is the experience.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured ureteral spasm mechanics and crystal growth dynamics |
| Material/Shader | Subsurface Scattering (SSS) + Crystalline Shader | Simulating renal tissue, crystal structure, and ureteral smooth muscle |
| Physics Engine | Rigid Body + Fluid Dynamics | Visualized stone migration, hydronephrosis pressure, smooth muscle spasm |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of kidney stone passage physiology |
Read more on Why Are Kidney Stones So Painful?
Pingback: Why Are Kidney Stones So Painful? The 3D Neuroscience Guide