The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why kidney stones are so painful — visualizing the neurological pain pathways activated by ureteral obstruction, the scientific comparison between renal colic and childbirth pain, and the specific mechanisms that make kidney stone pain uniquely intense among all human pain experiences. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why Are Kidney Stones So Painful? (The Atomic Answer)
Why are kidney stones so painful? The answer involves the simultaneous activation of multiple pain systems — producing an experience that is not simply “severe pain” but a physiologically unique combination of visceral colic, capsular stretch pain, and referred somatic pain that overwhelms the nervous system’s ability to process and localize it.
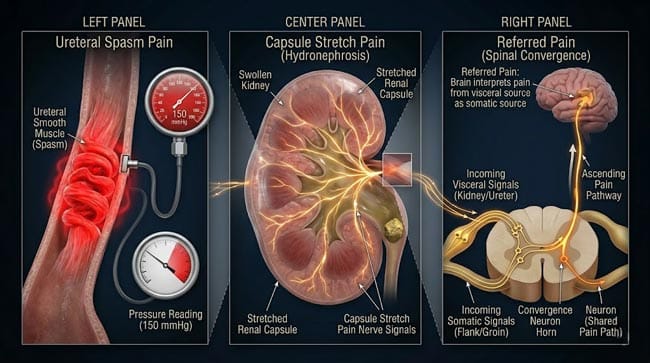
- Three Simultaneous Pain Sources: Kidney stone pain comes from three simultaneously activated sources: ureteral smooth muscle spasm (the primary source — shown producing the worst pain), renal capsule stretch from hydronephrotic pressure, and referred somatic pain from viscero-somatic convergence at the spinal cord.
- The Spasm Factor: Ureteral smooth muscle contractions during stone obstruction shown reaching pressures of 50–150 mmHg — compared to normal peristaltic pressure of 5–25 mmHg. This is 3–6 times the normal force — applied in uncoordinated, violent bursts.
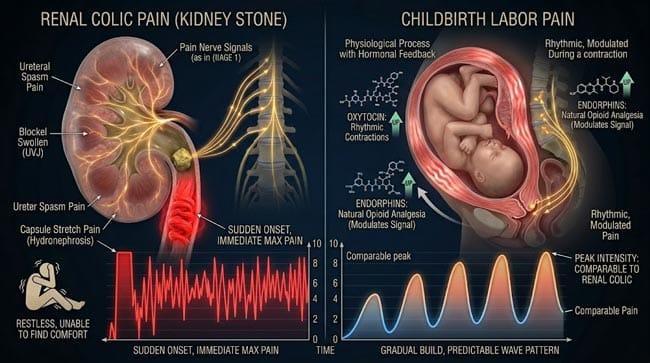
- The No-Warning Factor: Unlike most severe pain that builds gradually, renal colic shown reaching maximum intensity within minutes of onset — giving the nervous system no time to activate descending pain inhibition mechanisms.
- The Comparison: When directly compared in pain scale studies, renal colic shown scoring 8–10 out of 10 on standard pain scales — comparable to active labor contractions and surgical pain without anesthesia.

My 3D Discovery: Rendering the “Pain Convergence”
When I was building the pain pathway model for this simulation, the most neurologically fascinating element was the referred pain mechanism. In the 3D spinal cord model, I showed the T10–L1 segments where the ureteral visceral afferents shown entering the spinal cord — and the simultaneous activation of the somatic sensory neurons from the flank, groin, and testicle/labia at these same levels.
The result shown as a pain signal that the brain shown unable to precisely localize — the visceral and somatic signals shown converging on the same spinal cord neurons, shown as the brain receiving ambiguous information about the pain’s origin. This explains the characteristic radiation pattern of renal colic — from flank to lower abdomen to groin to genitalia — the brain shown projecting the pain to every somatic region that shares innervation with the ureter.
3D Observation: The most powerful visualization in this simulation is showing the patient’s pain experience from the brain’s perspective. The brain shown receiving simultaneous pain signals from: the ureter (visceral colic pain), the renal capsule (capsular stretch pain), and the shared somatic territories of T10–L1 (flank, abdomen, groin, scrotum/labia). The somatosensory cortex shown lighting up across an extraordinarily large area — the brain shown unable to determine precisely where the pain is coming from because it is genuinely coming from multiple sources simultaneously. The person shown experiencing pain that seems to be everywhere and nowhere — moving and shifting as the ureteral spasms change location and intensity.
Stage 1: The Three Pain Sources — Why Everything Hurts
Pain Source 1 — Ureteral Smooth Muscle Spasm:
This is the dominant pain generator in renal colic. In our 3D ureteral pain model:
Normal ureteral peristalsis shown producing pressures of 5–25 mmHg — sufficient to propel urine against gravity without pain.
Stone-obstructed ureteral spasm shown producing pressures of 50–150 mmHg — 3–6 times normal. This extreme pressure activates:
- Mechanoreceptors in the ureteral wall — shown as rapidly adapting pressure sensors shown being overwhelmed by the pressure magnitude
- C-fiber nociceptors — unmyelinated pain fibers shown throughout the ureteral adventitia — shown firing at maximum rate in response to the ischemia produced by the intense muscle contraction
- Prostaglandin production — ureteral ischemia shown triggering local prostaglandin release — shown as PGE2 molecules shown sensitizing the C-fibers and producing a feedback loop that amplifies the pain signal
The Spasm Character:
Ureteral spasms shown as not continuous — they shown occurring in waves, typically every 1–3 minutes — each wave shown lasting 20–60 seconds. This wave pattern shown producing the characteristic colicky (wave-like) quality of renal colic — pain shown building to a peak, partially subsiding, then building again. Between waves, the background ache from hydronephrosis shown persisting.
Pain Source 2 — Renal Capsule Stretch:
The kidney shown enclosed in a fibrous capsule — the renal capsule — that is richly innervated with pain fibers. When the ureter is obstructed, urine shown unable to drain — shown backing up and distending the collecting system. This hydronephrotic distension shown stretching the renal capsule — shown as a continuous, aching pain distinct from the colicky ureteral pain.
In the 3D renal pressure model:
- Normal intrarenal pressure: approximately 5–10 mmHg
- Acute complete ureteral obstruction: shown reaching 50–70 mmHg within hours
- Renal capsular stretch pain shown as described as a “deep, constant ache” in the flank — persisting between the colicky spasm episodes
Pain Source 3 — Referred Somatic Pain:
This is the most neurologically complex component of renal colic. In our 3D spinal cord model, I showed the viscero-somatic convergence mechanism:
The ureter’s visceral pain fibers shown entering the spinal cord at T10–L1 segments — the same segments that receive somatic sensory input from:
- T10: Lower abdomen
- T11–T12: Inguinal region, upper scrotum/labia
- L1: Inner thigh, testicle/labia majora
At the dorsal horn of the spinal cord, visceral pain neurons shown sharing interneurons with somatic pain neurons — shown as the gate control theory mechanism. When the visceral signal is intense enough, it shown “spilling over” to activate somatic pathways — shown as the brain shown misinterpreting the signal as coming from the somatic tissues.
The Result: The patient shown experiencing pain in the flank AND lower abdomen AND groin AND genitalia — simultaneously — because the visceral signal shown activating all shared somatic pathways at once.
| Pain Source | Mechanism | Character | Location | Intensity |
|---|---|---|---|---|
| Ureteral spasm | Ischemia + mechanoreceptors + C-fibers | Colicky, severe waves | Flank/ipsilateral back | 9–10/10 at peak |
| Renal capsule stretch | Hydronephrosis + capsular innervation | Constant deep ache | Costovertebral angle | 6–8/10 |
| Referred somatic pain | Viscero-somatic convergence at T10–L1 | Radiating, diffuse | Flank → groin → genitalia | Variable, 5–8/10 |
Stage 2: The Comparison — Kidney Stones vs. Childbirth
The Scientific Pain Comparison:
The claim that kidney stones are worse than childbirth is one of the most common pain comparisons in medicine — and it has been the subject of actual clinical research. In our 3D pain research model, I showed the data:
Renal Colic Pain Assessment: Multiple studies using validated pain scales (VAS — Visual Analog Scale, NRS — Numeric Rating Scale) shown renal colic producing scores of 8–10/10 consistently. In emergency department studies, shown as one of the highest-scoring pain presentations — comparable to myocardial infarction and postoperative pain.
Childbirth Pain Assessment: Active labor pain shown scoring 7–10/10 on VAS scales — with significant variability based on whether epidural analgesia is used, parity (first vs. subsequent births), and individual factors. In studies comparing unmedicated labor to other pain types, shown as typically slightly lower than the peak of renal colic in comparative studies — but with the important caveat that labor pain has a different character and temporal pattern.
Key Differences That Make Direct Comparison Difficult:
Duration: Labor pain shown lasting hours to days — with periods of less severe pain between contractions. Renal colic shown lasting hours typically — but shown as a more consistently severe experience with less inter-episode relief.
Predictability: Labor pain shown being anticipated and prepared for — descending pain inhibition (the endogenous opioid system) shown being activated through preparation, breathing techniques, and expectation management. Renal colic shown arriving without warning — descending inhibition shown having no time to activate.
Emotional Context: Labor pain shown occurring in a context of positive anticipation and purposeful suffering. Renal colic shown occurring as unexpected, purposeless suffering — the psychological component shown amplifying the pain experience significantly.
The Physiological Mechanism Differences:
In our 3D comparative pain model, I showed why the two pains feel different despite similar intensity ratings:
Childbirth uterine contractions:
- Source: Uterine smooth muscle contractions — similar mechanism to ureteral spasm but in a much larger organ
- Character: Strong contractions building to peak over 30–60 seconds, then releasing — predictable wave pattern
- Additional component: Perineal stretching during descent and delivery — somatic pain distinct from the visceral contraction pain
- Hormonal modulation: Oxytocin, endorphins, and bonding hormones shown modulating the pain experience significantly
Renal colic:
- Source: Ureteral spasm (much smaller organ, higher pressure per unit area) + capsular stretch
- Character: Less predictable, often more sustained at peak intensity
- Additional component: Nausea, vomiting, inability to find comfortable position (no position shown relieving visceral colic)
- Hormonal modulation: Minimal — no positive emotional hormones counterbalancing the pain
The “Writhing” Sign:
A clinically useful observation shown in our 3D model: patients with somatic pain (appendicitis, peritonitis) shown typically lying very still — movement shown worsening somatic pain. Patients with renal colic shown typically unable to stay still — shown constantly moving, pacing, shifting — because no position shown providing relief from visceral colic. This writhing pattern shown as a clinical diagnostic clue for ureteral stone pain.
Stage 3: The Brain’s Experience — How Pain This Severe Is Processed
The Ascending Pain Pathway:
In our 3D central nervous system model, I tracked the renal colic pain signal from ureter to conscious experience:
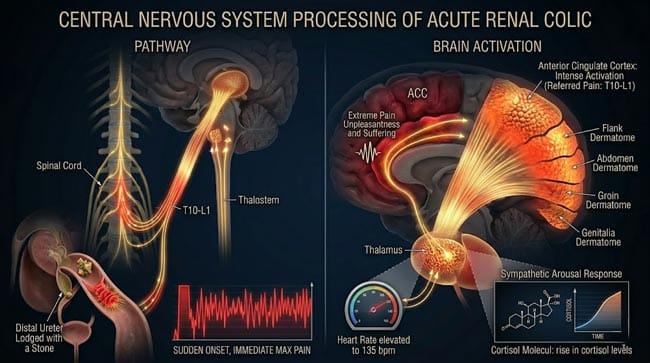
Spinal Cord (T10–L1): Visceral C-fibers and A-delta fibers shown entering the dorsal horn — synapsing on second-order neurons. The intense signal shown activating both the spinothalamic tract (discriminative pain — where is it?) and the spinoreticular tract (affective pain — how bad is it?).
The Thalamus: Second-order neurons shown ascending to the thalamus — the relay station for pain signals. The intensity of the signal shown triggering an arousal response — shown as the hypothalamus activating the sympathetic nervous system response: heart rate shown increasing, blood pressure shown rising, cortisol shown being released.
The Somatosensory Cortex: Third-order neurons shown projecting to the somatosensory cortex — shown attempting to localize the pain. The convergence of visceral and somatic signals shown making precise localization impossible — shown as an unusually large cortical activation zone corresponding to the T10–L1 dermatomes.
The Anterior Cingulate Cortex: The affective component of pain — “how unpleasant is this?” — shown being processed here. Renal colic shown producing extreme anterior cingulate activation — shown corresponding to the panic and distress that patients with severe renal colic uniformly report.
Why No Position Helps:
In our 3D position-pain model, I showed why patients cannot find relief in any position:
Somatic pain shown being modulated by position — lying still reduces movement of inflamed tissue. Visceral pain from hollow organ spasm shown not being modulated by position because the pain source is internal smooth muscle — no external position change shown affecting the ureteral spasm or hydronephrosis pressure. This shown as explaining the characteristic restlessness of renal colic patients — they move because instinct drives them to find relief that physiologically cannot exist in any position.
FAQ: Why Are Kidney Stones So Painful?
Q1: Is kidney stone pain really worse than childbirth? Direct comparison is scientifically complex — both pain types shown scoring similarly on validated pain scales (8–10/10 for both severe renal colic and active labor). Whether any individual experiences one as worse depends on their pain sensitivity, the size and location of the stone, whether analgesia is used during labor, and the psychological context. Many people who have experienced both shown reporting renal colic as worse — specifically because of its unpredictable onset, inability to find any comfortable position, and the absence of the positive emotional context that accompanies labor.
Q2: Why does kidney stone pain make some people vomit? Nausea and vomiting shown as extremely common with severe renal colic — occurring in over 50% of patients. The mechanism involves two pathways: the intense visceral pain signal shown activating the chemoreceptor trigger zone (CTZ) and nucleus tractus solitarius in the brainstem — the same centers involved in motion sickness and chemotherapy-induced nausea. Additionally, the vagal nerve shown carrying the visceral pain signal to the same brainstem nuclei that coordinate vomiting — shown as visceral pain directly activating the vomiting reflex.
Q3: Can you pass out from kidney stone pain? Yes — vasovagal syncope from extreme pain shown occurring with severe renal colic. The intense pain signal shown triggering a paradoxical vagal response — shown as heart rate and blood pressure shown dropping despite the normally sympathetic-activating nature of pain. This vasovagal response shown more likely in individuals with high vagal tone. Additionally, severe pain shown impairing vascular autoregulation — standing patients shown at risk of orthostatic hypotension from pain-induced sympathetic dysregulation.
Q4: Why does the pain sometimes stop suddenly? Sudden complete pain relief shown occurring for several reasons: the stone shown passing through a narrow point and reaching a wider segment of the ureter (temporarily less spasm), the stone shown passing into the bladder (immediate end of ureteral pain), or the obstructed kidney shown temporarily reducing urine production in response to high intrarenal pressure (reducing the hydronephrotic component). The sudden relief shown sometimes making patients believe the stone has passed — but pain recurrence shown if the stone shown still in the ureter.
Q5: Does size of the stone correlate with pain intensity? Counterintuitively — not always. A 2–3mm stone at the UVJ (ureterovesical junction) shown often producing MORE pain than a 5–6mm stone in the mid-ureter — because smaller stones shown fitting into narrow junctions more completely, causing more complete obstruction and more intense spasm. The pain intensity shown correlating more strongly with the degree of obstruction than with stone size — partial obstruction shown sometimes producing less pain than complete obstruction of the same size stone.
Conclusion: The Pain That Has No Position
Kidney stone pain occupies a unique place in human pain experience — not simply for its severity, but for its specific combination of features that makes it particularly difficult to endure. Rapid onset without warning. Inability to find relief in any position. Simultaneous activation of multiple pain systems. A colicky wave pattern that prevents adaptation or habituation. And the knowledge that the cause cannot be removed by rest, ice, or lying still.
In 3D, rendering the simultaneous activation of ureteral spasm pain, capsular stretch pain, and referred somatic pain pathways — and showing the brain attempting to localize a signal arriving simultaneously from three different sources — makes immediately clear why even people who have experienced significant pain from other causes often describe renal colic as uniquely distressing.
The stone is hard. The ureter is narrow. The nervous system has no adequate preparation for what happens when they meet.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured ureteral spasm pressure dynamics and central pain pathway activation |
| Material/Shader | Subsurface Scattering (SSS) | Simulating ureteral tissue, renal capsule, and neural pain pathway visualization |
| Physics Engine | Volumetric Particle System + Fluid Dynamics | Visualized prostaglandin sensitization, C-fiber activation, spinal cord convergence |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of renal colic pain neuroscience |
Read more on What Happens When You Pass a Kidney Stone?
Pingback: What Happens When You Pass a Kidney Stone? 3D Science Guide