The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why you should not clean ears with Q-tips — visualizing cerumen’s biological functions, cotton swab impaction mechanics, the self-cleaning anatomy of the ear canal, and what happens to the auditory system when earwax is pushed deeper rather than removed. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why You Should Not Clean Ears With Q-Tips? (The Atomic Answer)
Why you should not clean ears with Q-tips comes down to a fundamental misunderstanding of what earwax is, what it does, and how the ear actually cleans itself.
- The Misunderstanding: Most people treat earwax as waste — something dirty that needs to be removed. In reality, cerumen (earwax) is a sophisticated biological substance produced specifically to protect the ear canal — with antimicrobial, lubricating, and self-cleaning properties.
- The Mechanics Problem: A cotton swab inserted into the ear canal does not remove earwax — it removes the outermost layer while pushing the deeper, older wax further toward the eardrum, compacting it into an increasingly dense plug.
- The Self-Cleaning System: The ear canal has a built-in migration system — epithelial cells in the canal move outward from the eardrum at the same rate as fingernail growth, carrying cerumen with them. Q-tips disrupt this natural conveyor belt.
- The Risk: Beyond impaction, Q-tip insertion carries real risk of tympanic membrane perforation — particularly when inserted during a startle reflex or by children. Approximately 12,500 children are treated for Q-tip related ear injuries in US emergency rooms annually.

My 3D Discovery: Rendering the “Wax Wall” Formation
When I was building the cerumen impaction model for this simulation, the most visually striking sequence was watching the compaction process in time-lapse. Each Q-tip insertion shown removing a thin surface layer of soft, new cerumen — while simultaneously shown compressing the older, drier cerumen beneath into a progressively denser mass.
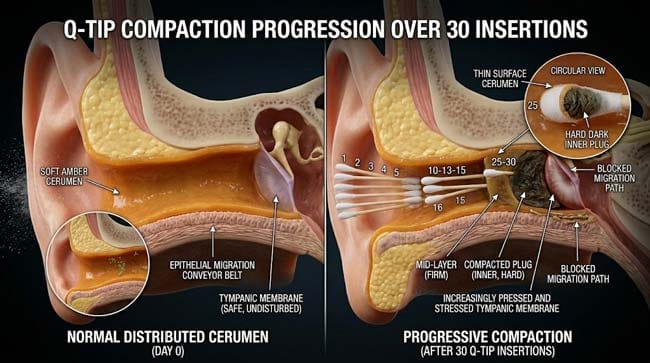
Over 30 simulated insertions (representing approximately one month of daily ear cleaning), the soft cerumen layer shown being repeatedly skimmed while the deep cerumen shown progressively compacting into a hard, dry plug that fills the inner ear canal and presses against the tympanic membrane.
3D Observation: The most counterintuitive visual in this simulation is showing the Q-tip’s net effect on total cerumen volume. A naive observer would expect repeated Q-tip use to reduce cerumen over time. The simulation shows the opposite — the soft surface layer is removed, but the compacted deep mass grows steadily larger and denser with each insertion. The Q-tip creates exactly the problem it is trying to solve, at a deeper and less accessible location.
Stage 1: What Earwax Actually Is — The Biology of Cerumen
Cerumen Is Not Waste — It Is a Biological Product:
Earwax is produced by two types of glands in the outer third (cartilaginous portion) of the ear canal:
Ceruminous glands — modified apocrine sweat glands shown as tubular coiled structures in the deep dermis of the canal wall. Produce the watery, protein-rich component of cerumen.
Sebaceous glands — oil-producing glands associated with hair follicles shown in the outer canal. Produce the lipid component of cerumen.
The combination creates cerumen — a complex emulsified mixture with a precise biological composition:
| Cerumen Component | Source | Biological Function | 3D Visualization |
|---|---|---|---|
| Long-chain fatty acids | Sebaceous glands | Antimicrobial barrier | Amber lipid layer |
| Cholesterol | Sebaceous glands | Membrane integrity | Crystalline structures |
| Lysozyme | Ceruminous glands | Enzyme that destroys bacterial cell walls | Green enzyme particles |
| Immunoglobulins (IgA) | Ceruminous glands | Antibody defense | Y-shaped proteins |
| Dead epithelial cells | Canal wall desquamation | Physical trap for debris | Pale flat discs |
| Keratin | Epithelial cells | Structural component | Fibrous matrix |
The Five Functions of Cerumen:
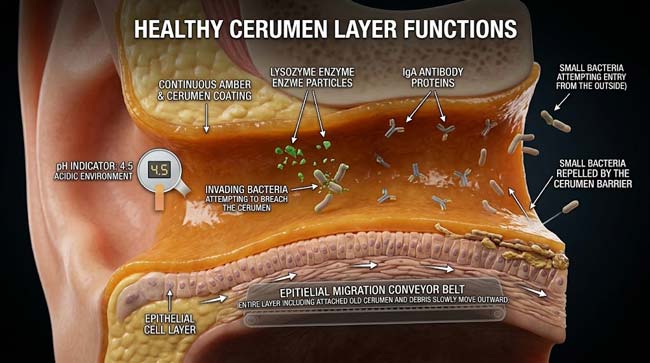
Function 1 — Antimicrobial Protection Cerumen maintains the ear canal at pH 4.5–6.5 — an acidic environment that inhibits the growth of bacteria and fungi. In our 3D model, the cerumen layer shown as a continuous acidic coating — bacteria contacting it shown being inhibited by both the low pH and the lysozyme enzyme content.
Without cerumen, the ear canal’s pH rises toward neutral — shown in the simulation as bacterial and fungal colonies now able to establish — explaining why excessive ear cleaning is associated with increased rates of otitis externa (swimmer’s ear).
Function 2 — Physical Trap The sticky, viscous properties of cerumen shown trapping dust, debris, insects, and small particles — preventing them from reaching the delicate tympanic membrane. In the animation, airborne particles shown becoming embedded in the cerumen layer rather than traveling deeper into the canal.
Function 3 — Lubrication The lipid content of cerumen lubricates the ear canal skin — preventing dryness, cracking, and itching. Shown as a continuous moisture barrier maintaining the canal epithelium’s integrity.
Function 4 — Water Repellency Cerumen’s hydrophobic properties shown repelling water — preventing moisture from reaching the inner canal where it could promote fungal and bacterial growth.
Function 5 — Self-Cleaning via Epithelial Migration This is the most remarkable and least understood function. The ear canal is the only skin surface in the body with directional epithelial cell migration — cells shown moving outward from the tympanic membrane toward the ear opening at approximately 1–2mm per week (the rate of fingernail growth).
In our 3D time-lapse migration model, I rendered individual epithelial cells shown migrating outward along the canal wall — carrying embedded cerumen, trapped debris, and dead cells with them. Over weeks, this migration shown transporting the entire cerumen contents of the canal from deep to superficial — a natural, passive cleaning system that requires no intervention.
According to the American Academy of Otolaryngology-Head and Neck Surgery, the ear is a self-cleaning organ — cerumen migrates naturally from the eardrum to the ear opening through the epithelial migration mechanism, and the vast majority of people never require manual ear cleaning of any kind. AAO-HNS: Cerumen Impaction Clinical Practice Guidelines
Stage 2: What Q-Tips Actually Do — The Impaction Mechanics
The Cotton Swab Paradox:
A Q-tip inserted into the ear canal does two things simultaneously — both shown clearly in our 3D mechanical simulation:
What it does at the surface (intended): The cotton tip shown contacting the soft, recently produced cerumen in the outer canal and absorbing or removing a small portion of this superficial layer.
What it does deeper (unintended and dominant effect): The cotton tip’s forward pressure shown pushing the leading edge of the cerumen column deeper into the canal — toward the tympanic membrane. The cerumen shown being compressed against the inner canal walls and the eardrum.
The Compaction Sequence:
In our 30-insertion time-lapse simulation, I tracked the total cerumen mass distribution over one month of daily Q-tip use:
Insertions 1–5: Soft superficial cerumen removed from outer canal. Deeper cerumen pushed 1–2mm deeper. Net effect: canal appears cleaner at the opening, but cerumen column slightly more compressed.
Insertions 6–15: Older, drier cerumen progressively compacted. The cerumen column shown becoming denser and harder. The outer canal shown feeling clean while the deep canal accumulates a growing mass.
Insertions 16–30: A distinct hard cerumen plug shown forming in the inner canal — dark, dry, and compressed against the tympanic membrane. The plug shown now too hard and deep for natural epithelial migration to remove. The patient shown experiencing early symptoms — muffled hearing, sensation of fullness, occasional tinnitus.
The Anatomy of Impacted Cerumen:
In our 3D cross-sectional model of cerumen impaction, I showed:
| Layer | Composition | Consistency | Distance from Eardrum |
|---|---|---|---|
| Outer (new) | Fresh cerumen, loose debris | Soft, honey-like | 15–20mm |
| Middle | Partially desiccated cerumen | Waxy, pliable | 8–15mm |
| Deep (impacted) | Desiccated, compacted cerumen | Hard, dry | 2–7mm |
| Core (worst cases) | Fully mineralized cerumen | Rock-hard | Against eardrum |
The Hearing Impact:
In our acoustic simulation, I modeled how progressively impacted cerumen affects sound transmission:
- Normal canal with appropriate cerumen: Sound transmission 95%+ of normal
- Mild impaction (50% canal occluded): Mild muffling, approximately 10–15 dB hearing reduction
- Moderate impaction (70% canal occluded): Noticeable hearing reduction, 20–30 dB loss
- Severe impaction (>90% canal occluded): Significant conductive hearing loss, 40+ dB reduction
The 3D acoustic model shown sound waves shown being progressively blocked by the cerumen plug — fewer and fewer waves reaching the tympanic membrane as impaction worsens.
According to the National Institute on Deafness and Other Communication Disorders (NIDCD), cerumen impaction affects approximately 6% of the general population and is one of the most common causes of reversible hearing loss — with Q-tip use being the primary contributing factor in the majority of cases. NIDCD: Earwax and Hearing
Stage 3: The Tympanic Membrane Risk — When Q-Tips Cause Serious Injury
The Perforation Risk:
The tympanic membrane sits at the end of the ear canal — approximately 25–35mm from the ear opening. A standard Q-tip is approximately 75mm long — meaning it is more than twice the length needed to reach the eardrum.
In our 3D geometric model, I showed the spatial relationship:
- Q-tip fully inserted: tip shown reaching the tympanic membrane with significant length to spare
- Q-tip at “safe” depth: shown with cotton tip still in contact with the cerumen column
- Q-tip during startle (sudden head movement): shown the tip shown moving an additional 5–10mm suddenly
The Perforation Sequence:
In our 3D tympanic membrane stress simulation, I modeled what happens when a Q-tip contacts the eardrum:
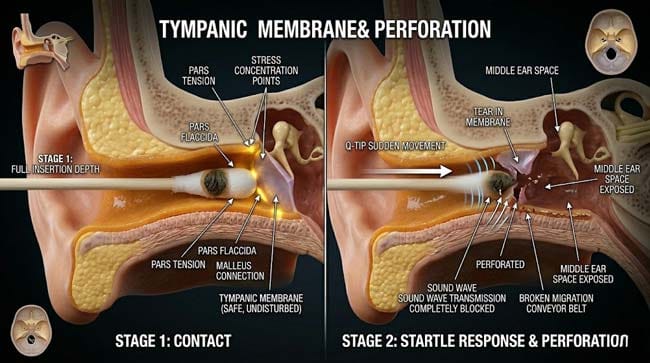
Gentle contact: The membrane shown deflecting inward under Q-tip pressure — the three-layer membrane structure shown under stress but maintaining integrity at low pressure.
Firm pressure: The membrane shown developing stress concentrations at its thinnest points — the central umbo region and the periphery near the annulus. At sufficient pressure, shown micro-tears beginning.
Startle or sudden insertion: Shown as the most dangerous scenario — the Q-tip shown moving suddenly, with the cotton tip shown penetrating the membrane before the deceleration reflex can activate. The perforation shown occurring in milliseconds.
The Statistics:
- Annual Q-tip related ear injuries in the US: approximately 12,500 children + significant adult cases
- Of these, approximately 73% involved tympanic membrane perforations
- Common triggers: child startling during insertion, another person bumping the Q-tip user, inserting while walking
After Perforation:
In our 3D post-perforation model, I showed:
- Immediate severe pain from tympanic membrane nerve supply activation
- Conductive hearing loss proportional to perforation size
- Risk of middle ear infection (otitis media) from exposed middle ear space
- Most small perforations (under 25% of membrane area) heal spontaneously within 4–8 weeks
- Large perforations may require surgical repair (tympanoplasty)
| Perforation Size | Hearing Loss | Spontaneous Healing Rate | Treatment |
|---|---|---|---|
| Small (<25% area) | 10–20 dB | >90% | Conservative, observation |
| Medium (25–50%) | 20–35 dB | 50–70% | Observation, possible patch |
| Large (>50%) | 35–50+ dB | <30% | Tympanoplasty likely needed |
FAQ: Why You Should Not Clean Ears With Q-Tips
Q1: How should you actually clean your ears if not with Q-tips? For most people — nothing. The epithelial migration system removes cerumen naturally. The only external cleaning needed is wiping the outer ear opening with a damp cloth during normal bathing. For people who produce excess cerumen or have naturally narrow canals, periodic use of over-the-counter cerumen softening drops (carbamide peroxide, mineral oil, or glycerin) followed by warm water irrigation is safe and effective. Professional ear syringing or microsuction by a healthcare provider is the safest option for established impaction.
Q2: Why do some people seem to need Q-tips because their ears produce so much wax? Some individuals naturally produce more cerumen — due to genetic factors, hearing aid use (which disrupts the normal outward migration), narrow or tortuous canal anatomy, or excessive use of earbuds. For these individuals, professional cerumen management every 6–12 months is appropriate. The solution is not Q-tips but rather cerumen softening drops used periodically and warm water irrigation — both of which work with rather than against the ear’s natural cleaning system.
Q3: Is it ever appropriate to use a Q-tip near the ear? Q-tips are useful for cleaning the visible outer ear — the folds and creases of the pinna (outer ear structure) that collect debris. The ear canal — the tube leading to the eardrum — is where Q-tips cause problems. The distinction is important: outer ear cleaning with a Q-tip is harmless, inner ear canal insertion is the behavior to avoid.
Q4: Why do ears feel cleaner after Q-tip use if the wax is just being pushed deeper? The Q-tip removes the superficial layer of soft cerumen — producing a genuine sensation of cleanliness at the outer canal entrance. The deeper compaction is invisible and painless until it becomes sufficiently severe to cause symptoms. This creates a deceptive feedback loop — the behavior feels effective because the outer canal feels clean, while the underlying problem progressively worsens. The sensation of cleanliness is real; the assumption that the ear has been properly cleaned is incorrect.
Q5: Can using Q-tips cause tinnitus? Cerumen impaction from chronic Q-tip use can cause tinnitus — typically described as a low-frequency rumbling or muffled sound — by altering the acoustic properties of the ear canal and affecting tympanic membrane tension. In most cases, this tinnitus resolves after professional cerumen removal. Tympanic membrane perforation from Q-tip trauma can also cause tinnitus — which may be temporary or, in cases of significant membrane damage, more persistent.
Conclusion: The Organ That Cleans Itself
The ear canal is one of the few body structures with a built-in, passive, continuous self-cleaning system — requiring no intervention, no tools, and no effort. The epithelial migration mechanism moves cerumen outward from the eardrum to the ear opening over weeks, carrying debris and dead cells with it, maintaining the optimal acoustic and microbial environment automatically.
In 3D, rendering the epithelial migration system — individual cells shown moving outward along the canal wall in a slow but continuous procession — makes the elegance of this mechanism immediately visible. And rendering the Q-tip compaction sequence alongside it makes equally clear why the intervention disrupts what the system is doing naturally.
The Q-tip is useful for many things. The ear canal is not one of them.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured epithelial migration mechanics and cerumen compaction dynamics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating ear canal tissue and cerumen viscosity at different desiccation levels |
| Physics Engine | Fluid Dynamics + Rigid Body | Visualized cerumen compaction, Q-tip pressure mechanics, acoustic wave blocking |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of cerumen biology and Q-tip impaction mechanics |
Read more on Q-Tip Ear Damage
Pingback: Q-Tip Ear Damage: The 3D Science of What Cotton Swabs Do