The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore what happens when you pop a pimple — visualizing follicle wall mechanics under pressure, bacterial spread into surrounding dermis, inflammatory cascade activation, and the scar formation process that follows traumatic follicle rupture. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Happens When You Pop a Pimple? (The Atomic Answer)
What happens when you pop a pimple is not what most people intend — and the actual sequence of events almost always makes the situation worse, not better.
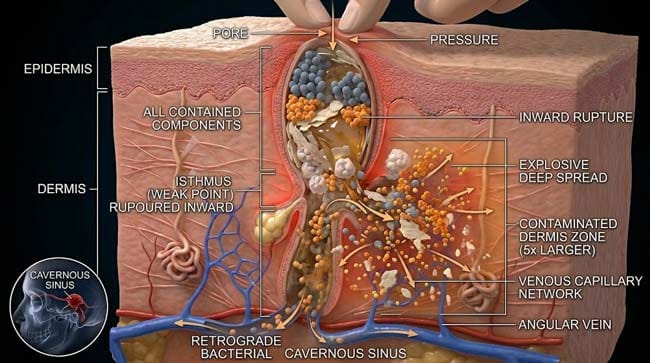
- The Pressure: Squeezing a pimple applies external pressure that forces the follicle wall to rupture — not upward and outward through the pore as intended, but often downward and sideways into the surrounding dermis.
- The Spread: When the follicle wall ruptures inward, infected contents — bacteria, keratin debris, sebum, and dead white blood cells — are injected directly into the surrounding dermis, creating a new, larger inflammatory zone.
- The Cascade: The dermis responds to this bacterial invasion with a massive inflammatory response — recruiting neutrophils, macrophages, and pro-inflammatory cytokines that produce more redness, more swelling, and more visible damage than the original pimple.
- The Scar: In the worst cases, the dermal collagen network is disrupted by the inflammatory response and subsequent repair process — producing the characteristic ice-pick, rolling, or boxcar acne scars that are far harder to treat than the original pimple.

My 3D Discovery: Rendering the “Wrong Direction” Problem
When I was building the follicle pressure model for this simulation, the most counterintuitive finding was the direction of rupture. Most people squeeze pimples expecting the infected contents to exit through the pore opening — upward and outward. In the 3D pressure simulation, this is rarely what actually happens.
The pore opening is the narrowest point of the follicle unit — surrounded by keratinized epithelium that provides significant mechanical resistance. The follicle wall in the mid-dermis, however, is significantly thinner and weaker — particularly at the isthmus (the narrow point between the infundibulum and the bulge region).
In the 3D viewport, when I applied squeeze pressure to an inflamed follicle, the first point of failure shown was consistently at the thin mid-dermal follicle wall — not at the pore opening. The infected contents shown forced through this weaker point — into the dermis — rather than through the pore.
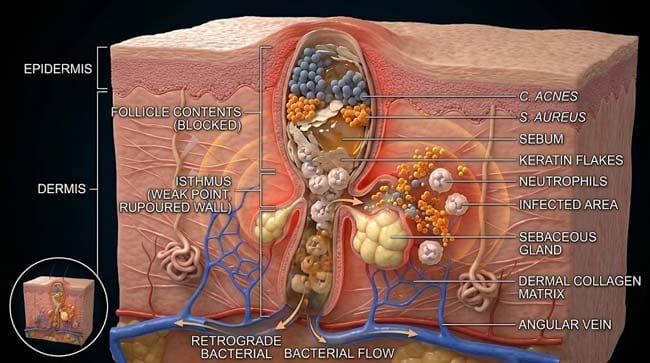
3D Observation: The most visually striking moment is the bacterial dispersal after follicle wall failure. The follicle contents — shown as a mixture of orange Staphylococcus aureus clusters, blue Cutibacterium acnes rods, pale keratin flakes, amber sebum droplets, and white neutrophil debris — do not exit cleanly. They explode into the surrounding dermis in multiple directions simultaneously. What was a contained bacterial infection within a follicle is now a dispersed bacterial contamination across a dermal area many times the size of the original pimple.
Stage 1: Inside a Pimple — What You Are Actually Squeezing
The Anatomy of an Inflamed Pimple:
Before understanding what happens when you pop a pimple, you need to understand what a pimple actually is at the microscopic level. In our 3D follicular model, I rendered a fully developed inflammatory papule/pustule in cross-section.
The Hair Follicle Unit: The pimple forms within the pilosebaceous unit — a hair follicle with its associated sebaceous (oil) gland. In the 3D model:
- Infundibulum — the upper portion of the follicle, connecting to the pore opening
- Isthmus — the narrow middle section — the mechanical weak point
- Lower segment — the deeper follicle containing the hair bulb
- Sebaceous gland — shown as a multi-lobed structure attached at the isthmus level
The Contents of an Inflammatory Pimple:
In our 3D content model, I rendered the precise composition of a typical inflamed pustule:
Cutibacterium acnes (formerly P. acnes) — shown as small blue-grey rods — the primary colonizing bacteria of the sebaceous follicle. C. acnes metabolizes sebum triglycerides into free fatty acids — shown as the metabolic byproducts that trigger the inflammatory cascade.
Staphylococcus epidermidis and S. aureus — shown as orange spherical clusters — secondary bacterial species that can colonize already-inflamed follicles.
Sebum — shown as amber viscous material — the oil produced by the sebaceous gland. Excess sebum production shown filling and distending the follicle.
Keratin debris — shown as pale flat discs — dead epithelial cells that have desquamated into the follicle lumen.
Neutrophils — shown as multi-lobed white blood cells — the primary immune responders that have infiltrated the follicle in response to bacterial signals. Dead neutrophils form the characteristic white/yellow pus.
Cytokines and inflammatory mediators — shown as small red particles — the chemical signals that maintain and amplify the inflammatory response.
The Follicle Wall Under Pressure:
In our structural model, I showed the follicle wall’s varying mechanical properties at different levels:
| Follicle Wall Location | Wall Thickness | Mechanical Strength | Rupture Risk Under Pressure |
|---|---|---|---|
| Infundibulum (upper) | Moderate | High (keratinized) | Low — pore resistance is high |
| Isthmus (mid-dermis) | Thin | Low (non-keratinized) | High — primary rupture point |
| Lower segment | Moderate | Moderate | Moderate |
| Sebaceous duct | Very thin | Very low | High secondary rupture point |
According to the American Academy of Dermatology, mechanical manipulation of inflamed acne lesions — including squeezing — is one of the primary causes of acne scarring and infection spread, with dermatologists consistently recommending against home extraction of inflammatory acne. AAD: Acne Treatment and Prevention
Stage 2: The Rupture Sequence — What Actually Happens When You Squeeze
The Pressure Mechanics:
In our 3D finite element pressure simulation, I modeled what happens to an inflamed follicle under typical finger-squeeze pressure:
Phase 1 — Initial Compression (0–0.5 seconds) External finger pressure shown compressing the surrounding skin tissue. The follicle shown as a pressurized vessel — the fluid contents shown transmitting pressure uniformly throughout the follicle space (Pascal’s principle).
Phase 2 — Pressure Buildup (0.5–1 second) As pressure increases, the follicle shown bulging at its weakest points — the isthmus region and any pre-existing micro-tears in the follicle wall. The pore opening shown remaining closed or minimally dilated — its keratinized walls providing significant resistance.
Phase 3 — Wall Failure (1–2 seconds) The isthmus wall shown failing at the point of maximum stress concentration — typically laterally rather than at the pore opening. The rupture shown occurring rapidly — a sudden failure rather than a gradual tear.
Phase 4 — Content Dispersal (2–5 seconds) Follicle contents shown released in multiple directions simultaneously:
- Upward (desired): Some material shown exiting through the pore — the intended outcome
- Lateral and downward (unintended): The majority of infected contents shown driven into the surrounding dermis through the rupture point
- Deep (worst case): Some material shown driven toward the deeper dermis and subcutaneous fat
The Dermal Contamination:
In the 3D dermal invasion model, I showed what happens immediately after follicle wall rupture:
Bacterial Dispersal C. acnes and S. aureus shown scattering into the dermis — colonizing new sites in the collagen matrix. Each bacterial cell shown as a potential new infection focus. From a single contained follicle infection, the rupture shown creating dozens of new bacterial micro-colonies scattered across a dermal area 5–10 times larger than the original pimple.
Keratin Foreign Body Response Keratin flakes shown dispersing into the dermis — where they are recognized as foreign material by dermal immune cells. Macrophages shown attempting to engulf keratin fragments — triggering a foreign body granulomatous response that can persist for weeks and contribute to deeper nodular lesions.
Sebum Saponification Free sebum in the dermis shown being acted upon by bacterial lipases — producing free fatty acids that are highly pro-inflammatory, shown as irritant particles triggering additional mast cell degranulation and neutrophil recruitment.
| Dispersed Component | Dermal Effect | Clinical Consequence | 3D Visualization |
|---|---|---|---|
| Bacteria (C. acnes, S. aureus) | New infection foci throughout dermis | Wider inflammatory zone, satellite lesions | Orange and blue particles dispersing |
| Keratin fragments | Foreign body granuloma response | Deep nodular lesions, prolonged inflammation | Pale discs triggering macrophage response |
| Sebum | Free fatty acid irritation | Amplified inflammation | Amber droplets producing cytokine cascade |
| Neutrophil debris | Additional inflammatory signals | Increased tissue damage | White cell fragments releasing enzymes |
| Cytokines | Regional immune activation | Surrounding skin involved in inflammation | Red particles spreading beyond original site |
Stage 3: The Inflammatory Cascade and Scar Formation
The Post-Rupture Inflammatory Response:
Following follicle wall rupture and dermal contamination, the immune system mounts a response significantly more intense than that directed at the intact follicle infection. In our 3D immune response model:
Hour 0–2: Mast Cell Degranulation Dermal mast cells shown detecting the sudden bacterial presence and keratin foreign bodies — shown as large granular cells releasing their contents (histamine, tryptase, pro-inflammatory mediators) shown as purple explosive bursts. This produces the immediate redness and swelling visible after squeezing.
Hour 2–12: Neutrophil Recruitment Shown as a massive influx of neutrophils — attracted by chemokines released from mast cells and bacteria-stimulated keratinocytes. Neutrophils shown arriving in numbers far exceeding those in the original intact follicle — attempting to contain the now-dispersed bacterial contamination.
Hour 12–48: Tissue Damage Neutrophils fighting dispersed bacteria shown releasing proteases and reactive oxygen species — shown as collateral tissue damage affecting collagen fibers and basement membrane in the surrounding dermis. This proteolytic tissue damage is the beginning of scar formation.
Days 2–14: Resolution or Scarring
Resolution pathway (mild cases): Macrophages shown clearing bacterial debris and dead cells. Fibroblasts shown beginning collagen synthesis to repair the dermal defect. The repaired area shown returning to near-normal architecture.
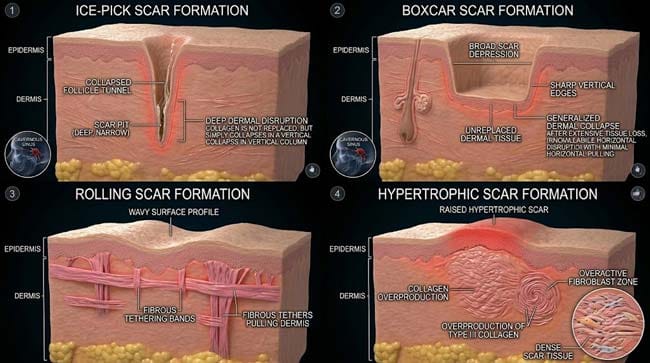
Scarring pathway (severe cases): The inflammatory response shown exceeding the tissue’s repair capacity. Three distinct scar patterns shown forming based on the repair response:
Ice-pick scars — shown as narrow, deep pits extending into the dermis. Formed when the follicle tunnel collapses and the overlying epidermis contracts downward as the dermal support is lost.
Boxcar scars — shown as broad, flat-bottomed depressions with sharp vertical edges. Formed when significant dermal collagen is destroyed in a defined area, leaving a depressed zone.
Rolling scars — shown as wave-like undulations across the skin surface. Formed when fibrous bands develop between the dermis and subcutaneous fat, tethering the overlying skin downward.
Hypertrophic/keloid scars — shown as raised, thickened tissue. Formed when fibroblasts overproduce collagen during repair — more common in darker skin types and on the chest/back.
| Scar Type | Formation Mechanism | 3D Visualization | Treatment Options |
|---|---|---|---|
| Ice-pick | Follicle tunnel collapse, epidermal contraction | Narrow deep pits in skin surface model | Punch excision, TCA cross |
| Boxcar | Dermal collagen destruction in defined area | Broad flat-bottomed depressions | Subcision, laser resurfacing |
| Rolling | Fibrous bands tethering skin to fat | Wave undulations on skin surface | Subcision, filler |
| Hypertrophic | Collagen overproduction | Raised thickened tissue | Steroid injection, laser |
FAQ: What Happens When You Pop a Pimple?
Q1: Why does popping a pimple sometimes make a bigger, more painful lump? This is the dermal contamination response described in Stage 2. When the follicle wall ruptures inward, the infected contents dispersed into the dermis trigger an immune response far larger than the original follicle infection. The result is a deep, painful inflammatory nodule — a nodulocystic lesion — that represents immune activity against dispersed bacterial and keratin debris throughout the dermis. This nodule contains no accessible pus (unlike the original pustule) because the contents are now scattered throughout the dermal tissue rather than contained in a follicle.
Q2: Does popping a pimple cause permanent damage every time? Not every pimple-popping event causes permanent scarring. Scarring depends on the depth of dermal damage, the intensity of the inflammatory response, and individual genetic factors affecting wound healing and collagen production. Small, superficial pimples that are squeezed with minimal trauma and resolve quickly are less likely to scar than deeply inflamed nodules. However, the risk of scarring is always present with mechanical manipulation, and the risk increases significantly with larger lesions and deeper follicle units.
Q3: Is it ever safe to pop a pimple? Dermatologists distinguish between different lesion types. A superficial whitehead (closed comedone) with a visible white head close to the surface, gently expressed with clean hands after softening in a warm shower, carries lower risk than squeezing a deep, painful, inflamed papule or nodule. However, even “safe” home extraction carries infection spread and scarring risk. Professional extraction by a dermatologist using sterile equipment and proper technique is always safer than home squeezing.
Q4: What should you do instead of popping a pimple? The most effective non-mechanical approaches: apply a warm compress to bring the pimple to a head (allowing natural drainage), use a topical benzoyl peroxide or salicylic acid spot treatment to reduce bacterial load and inflammation, apply a hydrocolloid bandage (pimple patch) which draws out fluid through osmosis without mechanical trauma, and allow the pimple to resolve naturally — which typically occurs within 3–7 days for a superficial lesion.
Q5: Can the bacteria from a popped pimple spread to other pores? Yes — this is one of the primary mechanisms behind acne clustering and the appearance of multiple new lesions after manipulation. The dispersed bacteria from a ruptured follicle contaminate surrounding skin and can colonize adjacent follicles — shown in the simulation as bacterial particles from the rupture site traveling through the surface sebum film and entering neighboring pore openings. This explains why touching, rubbing, or picking at acne lesions consistently increases the total number of active lesions in the affected area.
Conclusion: The Most Counterproductive Skincare Habit
Popping pimples is one of the most universally practiced and consistently counterproductive skincare behaviors. The instinct to remove something unsightly is entirely understandable. The biology of what actually happens — follicle wall failure in the wrong direction, bacterial dispersal into the dermis, immune over-response, and collagen destruction — consistently produces outcomes worse than the original pimple.
In 3D, watching the follicle wall fail at the isthmus rather than the pore, then tracking the infected contents as they scatter through the dermis triggering an immune response far larger than the original infection, makes the mechanism immediately clear. The pimple is not removed. The infection is redistributed.
The dermal collagen network that provides your skin’s structural support does not distinguish between bacterial damage and immune-mediated collateral damage. Both destroy it. Both produce scars. And scars, unlike pimples, do not resolve in a week.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured follicle wall rupture mechanics and bacterial dispersal dynamics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating skin tissue layers, follicle wall translucency, and dermal collagen |
| Physics Engine | Finite Element + Fluid Dynamics | Visualized pressure distribution, wall failure mechanics, content dispersal |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of pimple popping skin mechanics |
Read more on Why You Should Never Pop a Pimple in the Triangle of Death
Pingback: Why You Should Never Pop a Pimple in the Triangle of Death: The 3D Vascular Science -