The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore how the body removes inhaled particles — visualizing mucociliary transport mechanics, cough reflex dynamics, alveolar macrophage phagocytosis, and the complete airway clearance system from nasal cavity to alveoli. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: How Does Your Body Remove Inhaled Particles? (The Atomic Answer)
How does your body remove inhaled particles? Through one of the most sophisticated biological clearance systems ever evolved — operating continuously, automatically, and without any conscious effort on your part.
- The Escalator: The mucociliary escalator — billions of coordinated cilia beating in synchronized waves beneath a sticky mucus layer — transports trapped particles from the deepest airways back toward the throat at 4–20mm per minute.
- The Emergency Expulsion: The cough reflex generates airflow velocities of up to 500 mph at the glottis — the fastest air speed produced by any biological mechanism — to forcibly expel particles that evade the escalator.
- The Last Defense: Alveolar macrophages — specialized immune cells that patrol the lung’s air sacs — engulf and destroy particles that reach the deepest lung tissue, where the mucociliary escalator cannot reach.
- The Timeline: Most inhaled particles are cleared from the upper airway within 30–60 minutes. Particles reaching the alveoli may take days to weeks to be fully processed by macrophages.

My 3D Discovery: Rendering the “Invisible Escalator”
When I was building the mucociliary model for this simulation, the most technically challenging and visually rewarding element was rendering the coordinated cilia beat at scale. Individual cilia are invisible to the naked eye — but in the 3D viewport, showing millions of them beating in synchronized metachronal waves creates one of the most mesmerizing visualizations in this entire series.
The wave pattern is not random. Each cilium beats slightly out of phase with its neighbor — creating a propagating wave that moves in one direction only, always toward the throat. In the animation, the combined effect looks like a perfectly coordinated biological conveyor belt, moving everything on its surface steadily and inevitably toward expulsion.
3D Observation: The most striking moment in this simulation is the contrast between the apparent stillness of the airway from the outside and the extraordinary activity happening at the microscopic level. From a macroscopic view, your airway looks passive and static. At the cellular level, billions of cilia are in constant, coordinated motion — processing, trapping, and transporting material 24 hours a day. It is one of the most visually dramatic demonstrations of biological complexity hidden within apparent simplicity.
Stage 1: The Mucociliary Escalator — The Body’s Primary Clearance System
The mucociliary escalator is the respiratory system’s first and primary mechanism for removing inhaled particles. It operates continuously throughout the entire respiratory tract — from the nasal cavity down through the trachea and bronchi — and represents one of the most elegantly engineered biological transport systems in the human body.
The Two-Layer Mucus System
The escalator depends on a precisely engineered two-layer mucus structure:
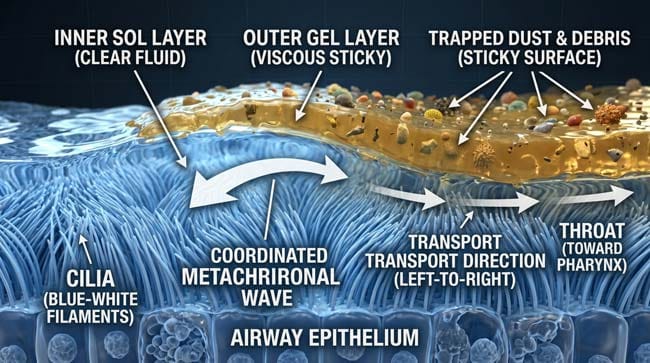
Sol Layer (Periciliary Layer) The inner layer — thin, watery, low-viscosity fluid that surrounds the cilia. In our 3D model, I rendered this as a clear, slightly shimmering fluid in which the cilia move freely. The sol layer allows cilia to complete their power stroke and recovery stroke without being impeded by the viscous gel above.
Gel Layer (Mucus Blanket) The outer layer — thick, viscous, gel-like mucus that forms a continuous blanket across the airway surface. Inhaled particles contact this layer and are immediately trapped. In the simulation, this appears as a golden semi-transparent surface that deforms around particles on contact — trapping dust, bacteria, pollen, insect particles, and other debris.
The Cilia Mechanics
Each ciliated cell has approximately 200 cilia on its surface. Each cilium performs a two-phase beat cycle:
Power Stroke (Forward) The cilium extends fully and sweeps forward through the gel layer — propelling the overlying mucus in the direction of the throat. In the 3D animation, this appears as a rapid, forceful forward sweep — the cilium shown pushing the golden mucus blanket forward by approximately its own length with each stroke.
Recovery Stroke (Backward) The cilium bends close to the cell surface — moving backward through the less viscous sol layer without dragging the gel layer back with it. In the animation, this appears as a slow, curved backward motion that resets the cilium for the next power stroke.
Metachronal Coordination Adjacent cilia beat slightly out of phase — creating the propagating wave pattern that gives the escalator its conveyor belt effect. In the 3D model, the offset timing between neighboring cilia creates a visible wave propagating continuously in one direction — always toward the throat.
| Escalator Component | 3D Visualization | Function | Specification |
|---|---|---|---|
| Sol layer | Clear shimmering fluid | Allows free cilia movement | 5–7 micrometers thick |
| Gel layer | Golden viscous surface | Traps inhaled particles | 2–5 micrometers thick |
| Cilia power stroke | Rapid forward sweep | Propels mucus toward throat | 10–15 beats per second |
| Cilia recovery stroke | Slow curved backward motion | Resets without dragging mucus back | Below sol layer surface |
| Metachronal wave | Propagating wave pattern | Creates directional transport | Continuous — 24 hours/day |
| Transport velocity | Moving carpet visualization | Moves particles toward pharynx | 4–20mm per minute |
Clearance Timeline by Airway Region:
| Airway Region | Cilia Density | Transport Speed | Clearance Time |
|---|---|---|---|
| Nasal cavity | Very high | 10–15mm per minute | 10–20 minutes |
| Trachea | High | 5–10mm per minute | 20–40 minutes |
| Main bronchi | High | 4–8mm per minute | 30–60 minutes |
| Small bronchi | Moderate | 2–4mm per minute | 1–4 hours |
| Bronchioles | Low | 1–2mm per minute | 2–6 hours |
| Alveoli | None | Macrophage-dependent | Days to weeks |
According to the American Thoracic Society, the mucociliary escalator clears approximately 10–100 grams of mucus from the respiratory tract per day in healthy adults — carrying with it all trapped particulate material, bacteria, and cellular debris that the respiratory system continuously encounters. ATS: Mucociliary Clearance in Health and Disease
Stage 2: The Cough Reflex — Emergency High-Speed Clearance
When the mucociliary escalator is insufficient — when a larger particle reaches the deeper airways, when mucus accumulates faster than cilia can transport it, or when an irritant directly contacts sensitive airway receptors — the cough reflex activates.
The cough is the respiratory system’s emergency clearance protocol — and in our 3D simulation, it is the most visually spectacular sequence.
The Cough Reflex Pathway:
Phase 1 — Sensory Detection Rapidly adapting receptors (RARs) and C-fiber receptors line the trachea, bronchi, and larynx. These receptors are exquisitely sensitive to mechanical stimulation, chemical irritants, and particle contact. When activated, they fire signals through the vagus nerve to the cough center in the brainstem.
In the 3D model, receptor activation appears as a bright pulse traveling along the golden vagus nerve from the airway to the brainstem — reaching the cough center in approximately 30 milliseconds.
Phase 2 — Deep Inhalation The cough center coordinates a rapid deep inhalation — shown in the animation as the diaphragm descending dramatically and the chest cavity expanding. This inhalation loads the lungs with approximately 2–3 liters of air above normal tidal volume — creating the pressure reservoir needed for explosive expulsion.
Phase 3 — Glottis Closure The vocal cords (glottis) close completely — shown as two folds of tissue sealing together in the 3D larynx model. Intrathoracic pressure builds rapidly as the respiratory muscles contract against the closed glottis.
Phase 4 — Explosive Expulsion The glottis opens suddenly. The simultaneous contraction of the diaphragm, intercostal muscles, and abdominal muscles produces an explosive expulsive force. In our 3D simulation, this generates an airflow particle system erupting through the glottis at velocities up to 500 mph (800 km/h) — producing a shockwave of air that physically propels particles from the airway walls back toward the mouth.
The 500 mph figure makes the cough one of the fastest biological airflow events in nature — exceeded only by some sneezing measurements in certain conditions.
Phase 5 — Particle Clearance The particle or mucus plug that triggered the cough is shown in the animation being physically entrained in the high-velocity airflow and expelled from the airway into the pharynx — where it is either expectorated or swallowed.
| Cough Phase | Duration | 3D Visual | Physical Event |
|---|---|---|---|
| Sensory detection | 0–30ms | Vagus nerve pulse to brainstem | Airway receptor activation |
| Deep inhalation | 0.5–1 sec | Diaphragm descending, chest expanding | 2–3L air reservoir loading |
| Glottis closure | Instantaneous | Vocal cords sealing | Pressure containment |
| Pressure buildup | 0.2–0.5 sec | Chest compression animation | 100–300 cmH₂O pressure |
| Explosive expulsion | 0.1–0.2 sec | 500 mph airflow particle burst | Particle clearance from airway |
Stage 3: Alveolar Macrophages — The Last Line of Defense
The mucociliary escalator and cough reflex handle particles in the conducting airways — the nasal cavity, trachea, bronchi, and bronchioles. But the deepest part of the lung — the alveoli (air sacs where gas exchange occurs) — has no cilia. Particles that reach this level require a completely different clearance mechanism.
Alveolar macrophages are the lung’s resident immune cells — specialized phagocytes that continuously patrol the alveolar surface, engulfing and destroying foreign particles, bacteria, and cellular debris.
How Alveolar Macrophages Work:
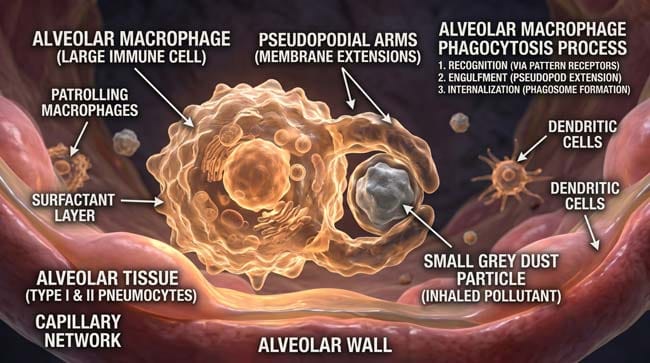
In our 3D alveolar model, I rendered macrophages as large, irregularly shaped cells that move slowly across the alveolar surface using pseudopodial extensions — arm-like projections that extend toward particles and pull them into the cell body.
Step 1 — Detection The macrophage detects the foreign particle through surface pattern recognition receptors — shown in the animation as receptor molecules on the cell surface binding to the particle’s surface characteristics.
Step 2 — Engulfment (Phagocytosis) The macrophage extends pseudopodia around the particle — shown as the cell membrane wrapping around and enclosing the object. The particle is pulled inside the cell body within a membrane-bound compartment called a phagosome.
Step 3 — Destruction The phagosome fuses with lysosomes — shown as small organelles containing digestive enzymes and reactive oxygen species. The combined compartment (phagolysosome) generates a toxic chemical environment that destroys biological particles — bacteria, insect fragments, organic debris.
Step 4 — Clearance The macrophage, now loaded with particle debris, moves toward the junction between alveolar and conducting airway tissue — shown in the animation as the cell slowly migrating to where the mucociliary escalator begins. The loaded macrophage is picked up by the escalator and transported to the throat, where it is eventually swallowed.
What Macrophages Can and Cannot Handle:
| Particle Type | Macrophage Response | Clearance Timeline | Outcome |
|---|---|---|---|
| Bacteria | Rapid phagocytosis and destruction | Hours to days | ✅ Eliminated |
| Insect fragments | Phagocytosis of small fragments | Days to weeks | ✅ Eliminated |
| Pollen | Phagocytosis | Days | ✅ Eliminated |
| Fine dust particles | Phagocytosis | Days to weeks | ✅ Mostly eliminated |
| Silica particles | Attempted phagocytosis — cell damage | Weeks to months | ⚠️ Chronic inflammation |
| Asbestos fibers | Cannot fully engulf — chronic response | Years | ❌ Permanent damage |
| Fine carbon particles | Partial — accumulates in macrophages | Decades | ⚠️ Visible as lung darkening |
According to the National Heart, Lung, and Blood Institute (NHLBI), alveolar macrophages are the primary defense against particles that penetrate to the alveolar level — with healthy adults maintaining a population of hundreds of millions of alveolar macrophages continuously patrolling the lung surface. NHLBI: Alveolar Macrophage Function

FAQ: How Does Your Body Remove Inhaled Particles?
Q1: Why do smokers cough more than non-smokers? Cigarette smoke contains thousands of chemical compounds that paralyze and destroy cilia — the primary transport mechanism of the mucociliary escalator. With cilia impaired, mucus and trapped particles accumulate in the airways. The body compensates by increasing cough frequency and intensity — using the emergency clearance system as the primary mechanism because the normal escalator is damaged. This is why smokers’ cough is chronic — the mucociliary system is continuously compromised.
Q2: Can your body remove all inhaled particles? For most particles encountered in normal daily life — pollen, dust, bacteria, small insects — yes. The mucociliary escalator and alveolar macrophages handle the vast majority of inhaled particles effectively. Certain particles — particularly very fine particles (PM2.5, less than 2.5 micrometers), asbestos fibers, and silica — can overwhelm or permanently damage these systems, leading to chronic lung diseases like silicosis, asbestosis, and pneumoconiosis.
Q3: How long does it take to clear inhaled pollen during allergy season? Pollen particles are typically 10–100 micrometers in size — too large to reach the alveoli and efficiently captured by nasal and bronchial mucus. In healthy individuals, pollen is cleared from the nasal cavity within 10–20 minutes by the mucociliary escalator. In allergy sufferers, the immune response to pollen — IgE antibody-mediated mast cell degranulation — causes inflammation that swells the nasal lining, reduces mucociliary transport efficiency, and produces the excessive mucus characteristic of hay fever symptoms.
Q4: Does exercising help clear your lungs of inhaled particles? Moderate exercise increases respiratory rate and depth, which increases airflow through the airways and may enhance mucociliary transport through increased mechanical stimulation of airway walls. Additionally, exercise-induced coughing can help clear accumulated mucus. However, exercising in heavily polluted air simultaneously increases the total particle load inhaled — potentially outweighing the clearance benefit.
Q5: Can breathing techniques like deep breathing improve lung clearance? Controlled deep breathing and breath-hold techniques are used therapeutically in pulmonary rehabilitation — particularly for conditions like cystic fibrosis and COPD where mucociliary function is impaired. Techniques like active cycle of breathing and autogenic drainage use controlled breathing patterns to mobilize mucus from small airways toward larger airways where coughing can expel it. For healthy individuals, normal breathing patterns maintain adequate mucociliary function without specific techniques.
Conclusion: The Invisible Army That Never Rests
Your respiratory system processes approximately 10,000 liters of air per day — every liter carrying dust, bacteria, pollen, pollutants, and occasionally an unfortunate insect. The fact that your lungs remain functional and clean throughout a lifetime of this continuous exposure is a testament to the extraordinary effectiveness of the mucociliary escalator, cough reflex, and alveolar macrophage system working in concert.
In 3D, rendering the complete clearance system — from the coordinated cilia wave in the nasal cavity to the macrophage slowly engulfing an alveolar particle — makes visible what is normally completely hidden. Billions of cilia beating continuously. Millions of macrophages patrolling silently. A cough mechanism capable of 500 mph airflows on demand.
The invisible army that keeps your lungs clean never takes a day off.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured cilia metachronal wave mechanics and macrophage phagocytosis dynamics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating airway mucosal tissue, mucus viscosity, and macrophage membrane |
| Physics Engine | Volumetric Particle System + Fluid Dynamics | Visualized cilia wave motion, cough airflow, and macrophage pseudopodial movement |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of complete respiratory particle clearance system |
Read more on What Happens If You Inhale a Bug?
Pingback: What Happens If You Inhale a Bug? 3D Nasal Defense Guide