The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore how a virus enters your body through breathing — visualizing aerosol particle dynamics, respiratory tract attachment mechanics, ACE2 receptor binding, and the critical window between viral entry and immune detection. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: How Does Virus Enter Your Body Through Breathing? (The Atomic Answer)
How does a virus enter your body through breathing? The process is faster, more precise, and more sophisticated than most people realize — and it begins the moment an infected aerosol particle contacts your respiratory tract.
- The Vehicle: Viruses travel through air inside aerosol particles — microscopic liquid droplets ranging from 0.1 to 100 micrometers in diameter, exhaled by infected individuals through breathing, speaking, coughing, and sneezing. Particles smaller than 5 micrometers remain airborne for hours.
- The Entry Point: Respiratory viruses target specific receptor proteins on airway cells — most famously the ACE2 receptor targeted by SARS-CoV-2, but also sialic acid receptors targeted by influenza and CD155 receptors targeted by certain enteroviruses.
- The Binding: Viral surface proteins lock onto these receptors with extraordinary precision — in our 3D simulation, the spike protein-ACE2 interaction looks like a perfectly engineered key sliding into a lock, triggering the cellular machinery that pulls the virus inside.
- The Critical Window: Between viral entry and immune detection, there is a window of 4–6 hours during which the virus replicates unchallenged — producing thousands of copies before the immune system receives its first alarm signal.

My 3D Discovery: Rendering the “Invisible Invasion”
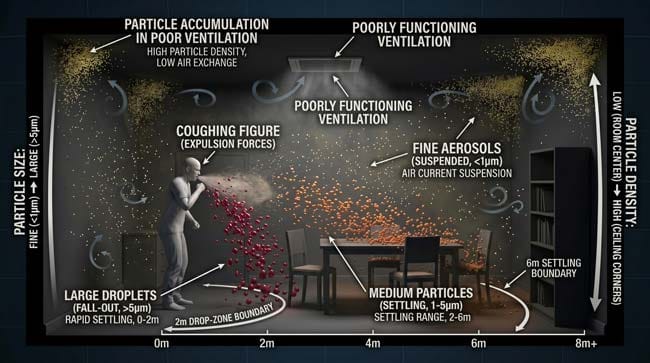
When I was building the aerosol particle model for this simulation, the most visually striking realization was just how long infectious aerosol particles remain suspended in indoor air. In the 3D fluid dynamics simulation, I modeled a single cough from an infected person in a typical indoor room — tracking where the aerosol particles traveled over the following hours.
The large droplets — shown as bright spheres — fell rapidly within 1–2 meters, landing on surfaces within seconds. But the fine aerosol particles — shown as tiny glowing points — remained suspended, drifting with air currents, spreading throughout the room, and maintaining infectious viral loads for up to 3 hours after the infected person had left.
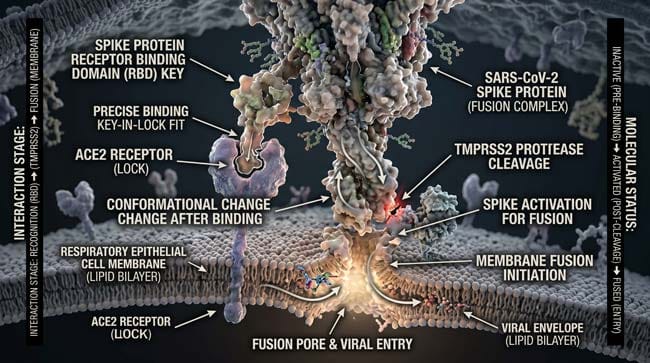
3D Observation: The most visually compelling moment in this simulation is the receptor binding sequence. In the molecular viewport, I rendered a single SARS-CoV-2 spike protein approaching an ACE2 receptor on a respiratory epithelial cell. The spike protein’s receptor binding domain shown rotating as it approaches — finding the precise orientation required for attachment. The moment it locks onto the ACE2 receptor, the cell’s own machinery begins pulling the virus inward. The cell is essentially helping the virus enter — because the virus has evolved to mimic the molecular signals the cell uses for legitimate nutrient transport.
Stage 1: The Aerosol — How Viruses Travel Through Air
Before a virus can enter your body through breathing, it must travel through air in a form that maintains infectivity. Understanding aerosol physics explains both how viral transmission works and why certain environments dramatically increase transmission risk.
Aerosol Particle Size and Behavior:
When an infected person exhales — through normal breathing, speaking, singing, coughing, or sneezing — they release respiratory secretions in a spectrum of particle sizes. In our 3D fluid dynamics model, I rendered this spectrum as particles color-coded by size:
Large Droplets (>100 micrometers) — Red particles Heavy enough to fall rapidly under gravity. In the simulation, these particles are shown falling in curved trajectories — hitting the floor or nearby surfaces within 1–2 seconds and 1–2 meters of the source. These droplets carry high viral loads but have limited range.
Medium Droplets (5–100 micrometers) — Orange particles Fall more slowly — remaining airborne for seconds to minutes before settling. Responsible for short-range transmission within approximately 2 meters.
Fine Aerosols (<5 micrometers) — Yellow particles So small they behave like gas molecules — remaining suspended in air for hours and traveling with air currents throughout an entire room or building. These are responsible for long-range airborne transmission and explain why infectious diseases can spread between people who never came into close contact.
Viral Load in Aerosols:
Not all aerosol particles carry equal viral loads. In our 3D model, I showed viral particle density within each droplet size category:
- Large droplets: High viral concentration but limited range
- Fine aerosols: Lower individual viral concentration but enormous in number and duration — collectively delivering significant viral exposure over extended periods
| Aerosol Type | Size | Airborne Duration | Range | Transmission Risk |
|---|---|---|---|---|
| Large droplets | >100 μm | Seconds | <2 meters | High at close range |
| Medium droplets | 5–100 μm | Minutes | 2–6 meters | Moderate |
| Fine aerosols | <5 μm | Hours | Entire room | High in enclosed spaces |
| Ultrafine aerosols | <1 μm | Days | Buildings | Moderate (lower viral load) |
Environmental Factors Affecting Aerosol Transmission:
In our environmental simulation, I modeled how different indoor conditions affect aerosol particle behavior and transmission risk:
- Poor ventilation — aerosol particles accumulate, shown as increasing particle density over time in a closed room
- High humidity — particles absorb moisture, grow larger, and fall faster — shown as particle trajectories shifting downward
- Low humidity — particles evaporate, shrink, and remain airborne longer — shown as extended suspension time
- Air filtration (HEPA) — particles captured by filtration, shown as particle density rapidly decreasing near filter units
According to the World Health Organization (WHO), respiratory viruses including SARS-CoV-2 and influenza are primarily transmitted through respiratory aerosols produced during breathing, speaking, coughing, and sneezing — with fine aerosol particles capable of remaining infectious in indoor air for extended periods. WHO: Airborne Disease Transmission
Stage 2: The Entry — How Viruses Attach to and Invade Respiratory Cells
Once an aerosol particle containing virus is inhaled, the virus must navigate the respiratory tract’s defense systems and find a susceptible cell to infect. This process is highly targeted — different viruses have evolved to attack specific cell types at specific locations in the respiratory tract.
The Respiratory Tract Entry Points:
Upper Respiratory Tract (Nose, Throat, Upper Airways) Most respiratory viruses first contact cells in the nasal cavity and nasopharynx — the passage connecting the back of the nose to the throat. These surfaces are lined with ciliated epithelial cells that express the receptor proteins targeted by respiratory viruses.
In our 3D model, the nasal cavity surface shown at cellular resolution — millions of epithelial cells displaying receptor proteins like antenna arrays on their outer surfaces. The ACE2 receptor, targeted by SARS-CoV-2, is shown as a specific protein configuration protruding from the cell surface.
Lower Respiratory Tract (Bronchi, Bronchioles, Alveoli) Viruses that evade upper respiratory defenses can reach the lower tract — where alveolar cells express high densities of the same receptor proteins. Lower respiratory tract infection is associated with more severe disease because gas exchange function is directly impaired.
The ACE2 Receptor — The Primary Lock:
The ACE2 (Angiotensin-Converting Enzyme 2) receptor is a protein present on the surface of cells throughout the respiratory tract — particularly in the nasal epithelium, bronchial cells, and Type II alveolar cells.
In our molecular simulation, I rendered the ACE2 receptor as a complex folded protein structure embedded in the cell membrane — shown as a specific three-dimensional shape that the viral spike protein is precisely complementary to.
The Binding Sequence (3D Molecular Detail):
Step 1 — Approach The virus — shown as a sphere covered in spike proteins — drifts toward the cell surface. The spike proteins shown rotating and sampling the cell surface, searching for ACE2 receptor configurations.
Step 2 — Initial Contact The spike protein’s receptor binding domain (RBD) makes contact with the ACE2 receptor. In the animation, this appears as the RBD — a specific domain of the spike protein — fitting into the ACE2 receptor’s binding groove with precise molecular complementarity.
Step 3 — Conformational Change ACE2 binding triggers a conformational change in the spike protein — shown as the protein reshaping dramatically, exposing a second domain (S2) that is required for membrane fusion. The cell’s own proteases (TMPRSS2) cleave the spike protein — activating the fusion mechanism.
Step 4 — Membrane Fusion The viral envelope fuses with the cell membrane — shown as the two lipid bilayers merging in a dramatic flowing animation. The viral contents — including the RNA genome — are released into the cell cytoplasm.
Step 5 — Viral RNA Release The viral RNA genome is now inside the cell — shown as a glowing strand uncoiling in the cytoplasm. The cell’s ribosomes begin translating viral proteins immediately — the invasion is complete.
| Entry Step | Duration | 3D Visual | Biological Event |
|---|---|---|---|
| Aerosol inhalation | Milliseconds | Particle entering airway | Virus contacts respiratory mucosa |
| Spike protein sampling | Seconds | Rotating spike proteins on cell surface | Receptor search |
| ACE2 binding | Seconds | RBD locking into receptor groove | High-affinity attachment |
| Conformational change | Seconds | Spike protein reshaping | Fusion activation |
| Membrane fusion | Minutes | Lipid bilayers merging | Viral contents enter cell |
| RNA release | Minutes | Viral genome uncoiling in cytoplasm | Infection established |
According to the National Institutes of Health (NIH), ACE2 receptor density varies significantly across different cell types and anatomical locations — with nasal epithelial cells showing particularly high ACE2 expression, explaining why the nasal cavity is a primary entry site for SARS-CoV-2 and related coronaviruses. NIH: ACE2 Expression in Respiratory Tract
Stage 3: The Critical Window — Hours Before the Immune System Responds
Once the virus has entered a respiratory cell and released its RNA genome, a critical period begins — the window between viral entry and immune system detection during which the virus replicates essentially unchallenged.
The Viral Replication Cycle:
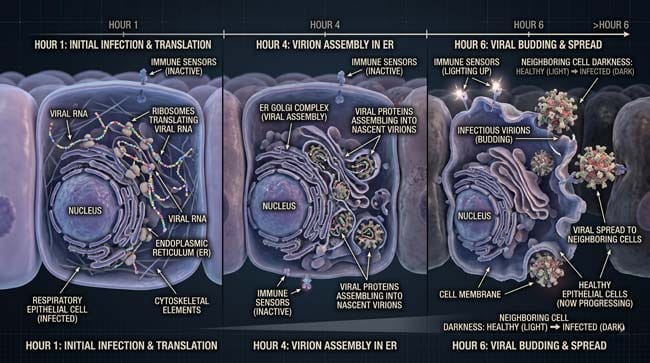
In our 3D cellular simulation, I rendered the complete replication cycle inside a single infected respiratory epithelial cell:
Hour 1 — Translation The viral RNA genome is read by the cell’s ribosomes — shown as molecular machines moving along the RNA strand and producing viral proteins. The cell is manufacturing viral components using its own cellular machinery — without any awareness that these are foreign proteins rather than its own.
Hour 2–4 — Assembly New viral components — RNA copies, spike proteins, envelope proteins, nucleocapsid proteins — are assembled in the endoplasmic reticulum and Golgi apparatus. In the animation, these organelles shown as manufacturing and packaging facilities — producing complete viral particles (virions) that accumulate within the cell.
Hour 4–6 — Release Assembled virions bud from the cell membrane — shown as new virus particles emerging from the cell surface, each coated in spike proteins ready to infect neighboring cells. A single infected cell can produce 100–1,000 new virus particles before immune detection.
Why the Immune System Takes Time to Respond:
The innate immune system detects viral infection through Pattern Recognition Receptors (PRRs) — molecular sensors that recognize specific viral signatures. However, many respiratory viruses have evolved mechanisms to delay or evade this detection:
- Interferon suppression — some viruses produce proteins that block interferon production, delaying the primary antiviral alarm signal
- Limited initial viral load — the very small number of viruses in a single inhaled aerosol particle may be below the detection threshold of PRRs for several replication cycles
- Intracellular replication — viruses replicate inside cells where extracellular immune sensors cannot detect them
In our 3D immune surveillance model, I showed the innate immune detection timeline — the PRR sensors shown as inactive during the first replication cycle, then beginning to activate as viral RNA accumulates to detectable levels around 4–6 hours after initial infection.
The Exponential Spread:
Once released from the first infected cell, new virions infect neighboring cells — shown in the simulation as an expanding wave of infection spreading across the respiratory epithelium. Each generation of infected cells produces more virus, infecting exponentially more cells — until the immune system finally mounts a detectable response.
| Time Post-Infection | Viral Event | 3D Visual | Immune Status |
|---|---|---|---|
| 0–1 hour | RNA translation begins | Ribosomes reading viral RNA | No detection |
| 1–4 hours | Viral assembly | ER and Golgi producing virions | No detection |
| 4–6 hours | First virion release | New particles budding from cell | PRRs beginning to activate |
| 6–12 hours | Exponential spread | Wave of infection across epithelium | Interferon production begins |
| 12–24 hours | Full innate response | Immune alarm signals spreading | Active immune response |
| 3–7 days | Adaptive response | T cells and B cells activating | Targeted immune response |
FAQ: How Does a Virus Enter Your Body Through Breathing?
Q1: How many viral particles does it take to cause an infection? The infectious dose varies dramatically between viruses. For norovirus, as few as 18 viral particles can establish infection. For influenza, the infectious dose is estimated at 100–1,000 particles. For SARS-CoV-2, estimates range from 100 to 1,000 particles depending on the variant and individual immune factors. A single cough can release millions of viral particles — making exposure in enclosed spaces with poor ventilation highly effective at delivering infectious doses.
Q2: Why do masks reduce transmission? Masks — particularly high-filtration masks like N95 respirators — reduce transmission through two mechanisms. First, they physically filter aerosol particles containing virus, reducing the number of viral particles reaching the respiratory mucosa. Second, they reduce the concentration of exhaled aerosols from infected wearers entering the shared air. N95 masks filter at least 95% of airborne particles ≥0.3 micrometers — significantly reducing both inhalation and exhalation of infectious aerosols.
Q3: Why do some people get infected and others do not after the same exposure? Multiple factors determine infection outcome after exposure: pre-existing immunity (from vaccination or prior infection), ACE2 receptor density and accessibility at airway entry points, innate immune response speed and effectiveness, viral load of exposure, and genetic factors affecting immune response genes. Some individuals have genetic variants in ACE2 or immune response genes that confer partial resistance to specific viruses.
Q4: Can viruses enter through the eyes? Yes — the conjunctiva (the membrane covering the eye surface) expresses ACE2 receptors and can serve as an entry point for respiratory viruses including SARS-CoV-2. Aerosol particles landing on the eye surface can initiate infection. The lacrimal duct connecting the eye to the nasal cavity also provides a direct anatomical pathway from conjunctival infection to nasal epithelial infection. This is one reason eye protection is recommended alongside respiratory protection in high-exposure environments.
Q5: How long can respiratory viruses survive in aerosols? Survival time in aerosols depends on the virus, humidity, temperature, and UV light exposure. SARS-CoV-2 has been shown to remain infectious in aerosols for up to 3 hours under controlled laboratory conditions. Influenza viruses survive in aerosols for 1–2 hours. Measles virus — one of the most highly transmissible respiratory viruses — can remain infectious in aerosols for up to 2 hours after an infected person has left the room. This is why measles can spread even without direct contact with an infected individual.
Conclusion: The Most Sophisticated Molecular Break-In
The process by which a respiratory virus enters your body through breathing is not random or crude — it is a precisely orchestrated molecular event refined over thousands of years of evolution. The virus has evolved to exploit the exact proteins your cells use for legitimate biological functions, to travel in aerosol particles that optimize airborne survival, and to replicate silently for critical hours before your immune system detects its presence.
In 3D, rendering the complete sequence — from aerosol particle dynamics to spike protein-ACE2 binding to viral RNA release inside the cell — makes visible a process that is invisible at human scale but defines the biology of respiratory illness at the molecular level.
Understanding this process at the 3D level transforms how we think about masks, ventilation, and the spaces we share with others — because the invisible mechanics of viral transmission are happening continuously in every enclosed space we occupy.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured aerosol particle dynamics and molecular binding mechanics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating respiratory epithelial tissue and viral envelope translucency |
| Physics Engine | Fluid Dynamics + Volumetric Particle System | Visualized aerosol behavior, receptor binding, membrane fusion |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of airborne viral entry mechanics |
Read more on How Does Your Body Fight Airborne Viruses?
Pingback: How Does Your Body Fight Airborne Viruses? 3D Immune Guide