The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore cola effects on teeth and bones — visualizing phosphoric acid enamel erosion mechanics, calcium phosphate dissolution, osteoclast activation from PTH signaling, and the progressive structural damage to dental and skeletal tissue from chronic cola consumption. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Are Cola’s Effects on Teeth and Bones? (The Atomic Answer)
Cola effects on teeth and bones operate through two distinct but related mechanisms — both driven by the same compound: phosphoric acid.
- On Teeth: Phosphoric acid directly attacks tooth enamel — the hardest substance in the human body — by dissolving the calcium phosphate crystals that give enamel its hardness. A single can of cola produces a measurable drop in oral pH to approximately 2.5–3.4, well below the 5.5 critical pH at which enamel begins dissolving.
- On Bones: Phosphoric acid absorbed into the bloodstream binds to calcium ions, reducing free blood calcium and triggering Parathyroid Hormone (PTH) release — which activates osteoclasts to dissolve bone and release calcium, progressively reducing bone mineral density.
- The Timeline: Enamel erosion from cola begins within minutes of the first sip. Measurable bone density reduction requires months to years of consistent high-volume consumption.
- The Compounding Effect: Unlike most dietary acids, phosphoric acid’s effects are not neutralized by saliva quickly — its strong acid nature means enamel dissolution continues for 20–30 minutes after each cola exposure.
My 3D Discovery: Rendering the “Invisible Dissolution”
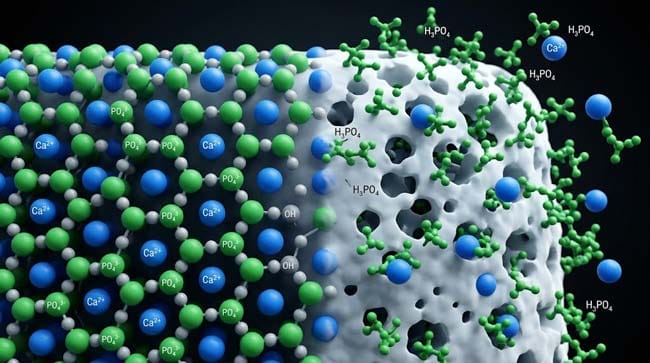
When I was building the enamel erosion model for this simulation, the most visually striking sequence was the time-lapse of enamel surface dissolution. At normal scale, a tooth looks smooth, white, and impervious. At the molecular level — the scale of our 3D simulation — it is a crystalline lattice of calcium phosphate hydroxyapatite, and when phosphoric acid contacts this lattice, the dissolution is immediate and dramatic.
In the 3D viewport, I rendered the enamel surface as a precisely ordered crystal structure — calcium ions shown as blue spheres, phosphate groups as orange tetrahedra, arranged in the repeating hydroxyapatite pattern. When I introduced the cola solution — shown as a wave of blue-green acid particles — the first thing visible is the acid molecules targeting the calcium ions at the crystal surface and pulling them out of position.
3D Observation: The most visually compelling moment in this simulation is watching the enamel crystal lattice dissolve at the molecular level. It does not dissolve uniformly — the acid attacks preferentially at crystal boundaries and surface defects, shown as specific dissolution points that spread progressively across the enamel surface. What begins as pinpoint dissolution sites expands over 20 minutes of acid exposure into visible surface pitting — the early stages of dental erosion that, over years, produces the characteristic smooth, scalloped enamel loss pattern seen in chronic cola drinkers.

Stage 1: Cola’s Effect on Teeth — The Acid Attack
Understanding Tooth Enamel
Tooth enamel is the hardest biological material in the human body — harder than bone, harder than most metals in terms of resistance to compression. Its hardness comes from its composition: hydroxyapatite — a crystalline calcium phosphate mineral (Ca₁₀(PO₄)₆(OH)₂) arranged in tightly packed prism structures.
In our 3D enamel model, I rendered this structure at atomic resolution — the hydroxyapatite crystal lattice shown as an extraordinarily dense, organized arrangement of calcium, phosphate, and hydroxyl groups. The beauty of the structure makes its vulnerability to acid all the more striking.
The pH Attack — How Cola Dissolves Enamel
Enamel begins dissolving at pH 5.5 — the critical demineralization threshold. Below this pH, the acid concentration is sufficient to begin pulling calcium and phosphate ions out of the hydroxyapatite crystal lattice.
Cola’s pH at consumption: approximately 2.5–3.4 — far below the 5.5 threshold.
For comparison:
| Beverage | pH | Enamel Risk |
|---|---|---|
| Pure water | 7.0 | None |
| Milk | 6.8 | None |
| Orange juice | 3.5–4.0 | Moderate |
| Cola (regular) | 2.5–3.4 | High |
| Diet cola | 3.0–3.7 | High |
| Battery acid | 1.0 | Extreme |
| Stomach acid | 1.5–3.5 | Extreme |
Cola sits in the same pH range as stomach acid — the fluid specifically evolved to dissolve biological tissue.
The Phosphoric Acid Dissolution Mechanism:
In our molecular simulation, I tracked the specific chemical reaction at the enamel surface:
Step 1 — Acid Contact Phosphoric acid (H₃PO₄) molecules shown making contact with the hydroxyapatite crystal surface. The acid’s hydrogen ions shown attacking the hydroxyl groups in the crystal structure.
Step 2 — Ion Extraction Hydrogen ions substitute for calcium in the crystal lattice — shown as H⁺ ions displacing Ca²⁺ ions from their crystal positions. The displaced calcium ions shown entering the surrounding solution as free ions.
Step 3 — Crystal Destabilization With calcium ions removed from their lattice positions, the surrounding crystal structure shown becoming unstable — adjacent crystal components beginning to shift and separate.
Step 4 — Progressive Dissolution The process shown accelerating as more surface area becomes exposed — the dissolution front expanding from initial contact points across the enamel surface, creating the characteristic etching pattern of acid erosion.
The 20-Minute Acid Window:
Unlike citric acid (found in orange juice), phosphoric acid is a stronger acid that produces a more sustained pH drop in the oral environment. In our oral pH simulation:
- Water: oral pH remains at approximately 7.0
- After cola sip: oral pH drops to approximately 3.0–3.5 within seconds
- Saliva buffering begins immediately but is insufficient to counter phosphoric acid rapidly
- Oral pH returns to safe levels (above 5.5) approximately 20–30 minutes after cola exposure
During this 20–30 minute window, enamel dissolution continues — meaning every sip of cola extends the erosion period rather than resetting it.
Sipping vs. Single Exposure:
In our time-exposure simulation, I compared two drinking patterns:
- Single glass consumed in 5 minutes: One 20–30 minute acid exposure period
- Sipping over 2 hours: Nearly continuous acid exposure — essentially eliminating the recovery time between exposures
This is why dentists consider sipping cola throughout the day significantly more damaging than drinking the same amount quickly — the pattern of exposure matters as much as the volume.
According to the American Dental Association (ADA), phosphoric acid in cola is one of the primary causes of dental erosion in adults — a condition affecting an estimated 1 in 3 adults and characterized by the loss of enamel surface that cannot be regenerated. ADA: Dental Erosion from Acidic Beverages
Stage 2: Cola’s Effect on Bones — The Calcium Depletion System
The bone effects of cola operate through a completely different mechanism than the direct acid attack on teeth — but the root cause is the same: phosphoric acid.
The Phosphate-Calcium Blood Chemistry:
When phosphoric acid is absorbed from the intestine into the bloodstream, it dissociates into phosphate ions (PO₄³⁻). These phosphate ions readily bind to free calcium ions (Ca²⁺) in the blood — forming calcium phosphate complexes that are not biologically active in the same way as free ionic calcium.
The body maintains blood calcium within an extraordinarily tight range (8.5–10.5 mg/dL) — deviations of even 10% trigger immediate hormonal responses.
The PTH Response Cascade:
In our 3D endocrine model, I rendered the complete PTH response sequence:
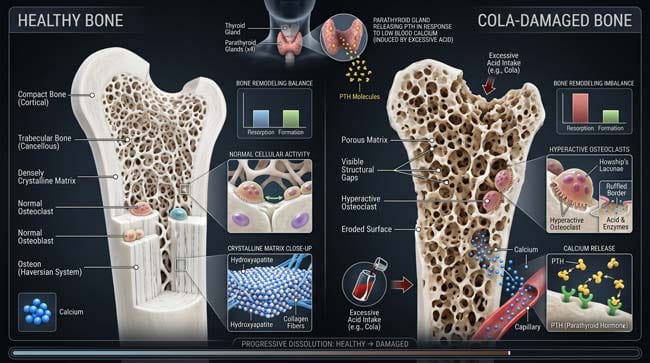
Step 1 — Calcium Drop Detection The parathyroid glands — four small glands on the posterior surface of the thyroid — continuously monitor blood calcium through calcium-sensing receptors (CaSR). When blood calcium falls below threshold, CaSR shown detecting the change and triggering rapid PTH secretion.
Step 2 — PTH Release PTH molecules — shown as small Y-shaped proteins — released into the bloodstream and traveling to three target organs simultaneously:
Step 3 — Bone Response PTH shown activating osteoclasts — large multinucleated cells that dissolve bone matrix. In the 3D bone model, osteoclasts shown attaching to bone surface and releasing acid (shown as yellow particles) and enzymes (shown as green particles) that dissolve hydroxyapatite, releasing calcium back into the blood.
Step 4 — Kidney Response PTH shown increasing calcium reabsorption in kidney tubules — reducing calcium lost in urine. Paradoxically, PTH also shown increasing phosphate excretion in urine — as the kidney attempts to reduce blood phosphate load.
Step 5 — Intestinal Response PTH shown stimulating Vitamin D activation — which increases intestinal calcium absorption. However, this mechanism requires dietary calcium to be available, which may be limited on a cola-only diet.
The Net Bone Effect:
| PTH Action | Short-term | Long-term (Chronic Cola) | 3D Visual |
|---|---|---|---|
| Osteoclast activation | Temporary calcium mobilization | Progressive bone loss | Osteoclasts shown dissolving bone |
| Kidney phosphate excretion | Phosphate reduction | Chronic PTH elevation needed | Kidney tubules excreting phosphate |
| Bone remodeling balance | Normal turnover | Osteoclast dominance | Bone density progressively reducing |
| Bone mineral density | Maintained short-term | Declining over months/years | Bone matrix becoming increasingly porous |
The Gender Difference in Cola-Related Bone Loss:
Clinical research shows women — particularly postmenopausal women — experience significantly greater cola-related bone density reduction than men. In our 3D comparative model, I showed two factors:
- Women have lower baseline bone density reserves than men
- The combination of cola consumption and estrogen decline (which normally protects bone) creates a compounding bone loss effect
The simulation shows bone density decline accelerating in the postmenopausal model — the same cola consumption producing measurably more bone loss than in the male equivalent model.
According to the National Osteoporosis Foundation, cola consumption is a documented modifiable risk factor for osteoporosis — with the phosphoric acid-calcium depletion mechanism explaining why cola-specific effects exceed those of other carbonated beverages that do not contain phosphoric acid. NOF: Calcium and Bone Health
Stage 3: The Combined Effect — When Teeth and Bones Are Attacked Simultaneously
In exclusive cola consumption — or chronic high-volume cola drinking — the dental and skeletal effects occur simultaneously, creating a compounding physiological picture.
The Dual Calcium Depletion:
Both mechanisms draw calcium from different compartments:
- Dental erosion removes calcium directly from tooth enamel — lost permanently, as enamel cannot regenerate
- Skeletal depletion removes calcium from bone matrix — partially reversible with adequate calcium intake and cessation of cola consumption
In our combined visualization, I showed both processes occurring simultaneously in a cola-heavy diet — the enamel slowly thinning from direct acid contact while the bone shown progressively losing density from the systemic phosphate-calcium cycle.
The Saliva Factor — Your Natural Defense:
Saliva plays a critical role in enamel defense — buffering oral pH and providing minerals for enamel remineralization. In our oral chemistry model:
- Saliva contains calcium and phosphate ions that can replenish dissolved enamel minerals during acid-free periods
- Saliva’s bicarbonate buffering system shown neutralizing acid after cola exposure
- Fluoride — from toothpaste or fluoridated water — shown enhancing remineralization by incorporating into the enamel crystal structure as fluorapatite (more acid-resistant than hydroxyapatite)
The Critical Balance:
- With adequate saliva flow and sufficient acid-free recovery time between cola exposures → enamel can partially remineralize between attacks
- With frequent sipping, dry mouth conditions, or very high-volume consumption → dissolution exceeds remineralization → net permanent enamel loss
The Timeline of Visible Damage:
| Duration of High Cola Consumption | Dental Changes | Bone Changes | 3D Visualization |
|---|---|---|---|
| Days–Weeks | Mild enamel softening, increased sensitivity | No measurable bone change | Surface crystal disruption visible |
| Months | Visible enamel thinning, altered tooth color | Early PTH elevation, borderline bone density | Surface erosion pattern developing |
| Years | Significant enamel loss, visible tooth shape change | Measurable bone density reduction | Characteristic scalloped erosion visible |
| Decades | Severe erosion, possible dentin exposure | Osteopenia to osteoporosis risk | Extensive structural dental and skeletal damage |

FAQ: Cola Effects on Teeth and Bones
Q1: Is diet cola better or worse for teeth than regular cola? Diet cola is equally damaging to tooth enamel as regular cola — and in some formulations, slightly worse. The phosphoric acid content is essentially identical between regular and diet versions. Diet cola’s lower sugar content actually makes it slightly more erosive in some measurements — sugar in regular cola partially occupies acid binding sites, marginally reducing acid contact with enamel. For teeth, the acid content is the primary determinant, not the sugar content.
Q2: Can you reverse cola-related enamel erosion? No. Tooth enamel is produced by ameloblast cells — which die after tooth formation is complete. Once enamel is lost, it cannot be regenerated by the body. Minor enamel softening can be partially remineralized by saliva and fluoride if caught early, but structural enamel loss is permanent. This is why dental erosion prevention — through reduced acid exposure and adequate remineralization — is far more important than treatment after the fact.
Q3: Does milk after cola help protect teeth? Consuming milk after cola can raise oral pH and provide calcium and phosphate ions that support enamel remineralization. However, this benefit is limited if the cola acid has already been active for 20–30 minutes before milk consumption. The most effective protective strategy is reducing the duration of acid exposure — drinking cola quickly rather than sipping and using fluoride toothpaste to support remineralization in the hours after exposure. Wait at least 30 minutes after cola before brushing — brushing immediately after acid exposure removes softened enamel.
Q4: Does sparkling water cause the same bone and tooth damage as cola? No — this is an important distinction. Sparkling water’s carbonic acid (from dissolved CO₂) is a much weaker acid than phosphoric acid — with a pH typically between 4.5–5.5 (vs cola’s 2.5–3.4). At this pH, carbonic acid is at or above the enamel critical threshold for most people and causes minimal erosion with normal consumption. Sparkling water also contains no phosphoric acid — meaning no calcium-binding blood phosphate effect and no PTH-driven bone calcium mobilization. Plain sparkling water is substantially safer for both teeth and bones than cola.
Q5: How much cola is safe to drink without significant dental or bone risk? There is no fully safe threshold — any cola consumption produces some acid exposure and some phosphate-calcium interaction. However, risk becomes clinically significant with chronic high-volume consumption. Current evidence suggests that limiting cola to occasional consumption (1–3 times per week), drinking quickly rather than sipping, following with water or milk, and maintaining adequate calcium intake can substantially mitigate both dental and bone risks. The critical behaviors are avoiding constant sipping throughout the day and ensuring adequate dietary calcium to compensate for cola-driven losses.
Conclusion: The Most Beautiful Crystal Being Slowly Dissolved
Tooth enamel is a biological masterpiece — the hardest substance produced by any living organism, arranged in a crystalline structure so precise it rivals engineered materials. The bone matrix is a living scaffold of similar mineral sophistication, continuously renewed and maintained by competing cellular forces.
Cola contains a single ingredient — phosphoric acid — that systematically attacks both structures simultaneously, through different mechanisms, at different timescales. The enamel attack is immediate and direct. The bone attack is hormonal and systemic.
In 3D, watching phosphoric acid molecules pull calcium ions from the hydroxyapatite crystal lattice — and separately watching osteoclasts dissolve bone under PTH stimulation from the same phosphate — reveals why a can of cola is uniquely damaging to hard tissues in a way that no other common beverage is.
The damage is invisible until it is not. And by the time it is visible — thinned enamel, scalloped tooth surfaces, reduced bone density on a scan — the loss is permanent.
Enjoy cola occasionally. Protect your enamel and your bones with everything between.
Further Study & External Research
- ADA — Dental Erosion from Acidic Beverages
- National Osteoporosis Foundation — Calcium and Bone Health
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured hydroxyapatite crystal dissolution and osteoclast bone erosion |
| Material/Shader | Subsurface Scattering (SSS) + Crystalline Shader | Simulating enamel crystal structure and bone matrix porosity changes |
| Physics Engine | Molecular Dynamics + Rigid Body | Visualized acid-crystal interaction, calcium ion displacement, osteoclast mechanics |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of cola phosphoric acid effects on dental and skeletal tissue |
Read more on What Happens If You Drink Only Cola?
Pingback: What Happens If You Drink Only Cola? The 3D Dehydration Science