The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore mushroom poisoning symptoms — visualizing the progressive stages of Amanita phalloides amatoxin damage, liver cell destruction mechanics, and the critical intervention timeline that determines survival. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Are Mushroom Poisoning Symptoms? (The Atomic Answer)
Mushroom poisoning symptoms are deceptive by design — the most dangerous species produce the least warning. Understanding the symptom timeline is the difference between survival and organ failure.
- The Silent Phase: The deadliest mushroom toxins — amatoxins from Amanita phalloides — produce zero symptoms for 6–24 hours after ingestion, while silently destroying liver cells at the molecular level.
- The Four Phases: Amatoxin poisoning progresses through four distinct clinical phases — Latent (silent damage), Gastrointestinal (first symptoms), False Recovery (dangerous improvement), and Hepatorenal Failure (organ collapse).
- The False Recovery Trap: Between approximately 24–48 hours, many patients feel significantly better — GI symptoms resolve and they believe they are recovering. In reality, this is the period of maximum liver destruction. This false recovery phase causes many patients to delay seeking treatment until it is too late.
- The Critical Window: Aggressive medical intervention within the first 24–36 hours significantly improves survival. After 72–96 hours without treatment, liver transplant becomes the only life-saving option.
My 3D Discovery: Rendering the “False Recovery” Deception
When I was building the four-phase symptom model for this simulation, the most unsettling sequence was the False Recovery phase. In the 3D viewport, I showed the body’s external symptoms resolving — the GI distress fading, the patient appearing to stabilize — while simultaneously showing the liver at the cellular level experiencing its most intense period of destruction.
The contrast between the external view and the internal view is the most powerful visual in this entire simulation. From the outside, the patient looks like they are getting better. Inside, the liver is losing 50–70% of its functional hepatocytes.
3D Observation: I rendered this using a split-screen visualization — left side showing a human figure with fading GI distress indicators, right side showing a cross-section of liver tissue with cells rapidly darkening and rupturing. The patient does not know what is happening inside. Without blood tests showing rapidly rising liver enzymes, there is no way to detect the internal catastrophe. This is why the False Recovery phase is so dangerous — and why anyone who has potentially ingested a toxic mushroom must remain under medical observation even when they feel fine.

Stage 1: The Four Clinical Phases — A Complete Symptom Timeline
Amatoxin poisoning — the most clinically significant form of mushroom poisoning — is unique in medicine for its four-phase progression. Understanding each phase explains both why patients often present to hospitals too late and why the symptom timeline is the most important diagnostic tool.
Phase 1 — The Latent Phase (0–6 to 24 hours)
What is happening internally: Alpha-Amanitin is being actively transported into hepatocytes (liver cells) by OATP (Organic Anion Transporting Polypeptide) transporters. Once inside, it binds irreversibly to RNA Polymerase II. Protein synthesis halts. DNA repair ceases. Cell death begins.
What the patient feels: Nothing. Completely asymptomatic.
In the 3D liver model, this phase shows a progressive darkening of hepatocytes — cell by cell — while external symptom indicators remain completely flat. The contrast between internal destruction and external normality is total.
Why this phase is so dangerous: The 6–24 hour asymptomatic window means that patients who ate a suspicious mushroom for dinner feel fine the next morning and do not seek medical care. By the time symptoms appear, significant irreversible hepatocyte death has already occurred.
Clinical note: Any person who has potentially consumed a wild mushroom — even if completely asymptomatic — should seek emergency evaluation immediately. Blood tests showing elevated ALT and AST (liver enzymes) can detect hepatocyte death before any symptoms appear.
Phase 2 — The Gastrointestinal Phase (6–24 hours)
What is happening internally: Sufficient hepatocyte death has occurred to produce systemic toxin effects. Intestinal epithelial cells — also high-turnover cells with significant RNA Polymerase II activity — begin failing. Inflammatory mediators are released.
What the patient feels:
- Sudden onset severe nausea and vomiting
- Profuse watery diarrhea (can be cholera-like in severity)
- Severe abdominal cramping
- Rapid dehydration from fluid loss
In the 3D gut model, the intestinal epithelial layer shown in Phase 1 as intact begins showing gaps — cells failing to replicate as protein synthesis collapses. The inflammatory response floods the intestinal tissue with immune cells, shown as a wave of red particles arriving at the mucosal surface.
The diagnostic trap: The GI symptoms of amatoxin poisoning are identical to many common foodborne illnesses — gastroenteritis, food poisoning, viral illness. Many patients and even physicians initially attribute these symptoms to something else entirely. The critical clue is the timing — onset 6–24 hours after a meal containing wild mushrooms.
| GI Symptom | Severity | Duration | 3D Mechanism |
|---|---|---|---|
| Nausea/vomiting | Severe | 12–24 hours | Intestinal epithelial failure + toxin-induced emesis reflex |
| Diarrhea | Profuse, watery | 12–24 hours | Intestinal lining breakdown, secretory failure |
| Abdominal pain | Severe cramping | 12–24 hours | Inflammatory mediator release, smooth muscle spasm |
| Dehydration | Significant | Ongoing | Fluid loss from vomiting and diarrhea |
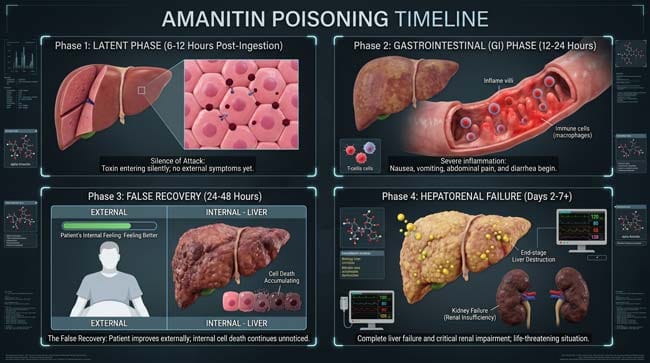
Phase 3 — The False Recovery Phase (24–72 hours)
What is happening internally: This is the most destructive phase of the entire poisoning sequence. The GI symptoms resolve as intestinal cells temporarily stabilize. The patient feels subjectively better — sometimes dramatically so. Meanwhile, hepatocyte destruction is at its absolute peak. 50–70% of liver cells may be destroyed during this phase.
What the patient feels:
- GI symptoms significantly reduced or resolved
- Feeling of overall improvement
- Some patients feel nearly normal
In the 3D split-screen model, this phase is the most visually striking. External symptoms: resolving. Internal liver: catastrophic destruction. The hepatocyte population shown as a dense field of healthy pink cells in Phase 1 now appears as a landscape of dark, collapsed, ruptured cells interspersed with the remaining survivors desperately attempting to maintain function.
The clinical emergency of Phase 3: Blood tests during this phase show dramatically elevated liver enzymes (ALT, AST may reach 1,000–10,000+ IU/L, versus normal <40 IU/L), rising bilirubin (causing jaundice), and declining coagulation factors (the liver produces clotting proteins — as it fails, bleeding risk escalates).
Why patients die from this phase: Patients who feel better during Phase 3 often leave hospitals against medical advice, believing they have recovered. They return in Phase 4 in fulminant liver failure, beyond the transplant assessment window.
According to the American Liver Foundation, amatoxin poisoning during the False Recovery phase is one of the most dangerous medical scenarios precisely because subjective improvement masks objective deterioration — making clinical monitoring of liver enzymes and coagulation markers essential even when the patient reports feeling well. American Liver Foundation: Toxic Liver Disease
Phase 4 — The Hepatorenal Failure Phase (72–96+ hours)
What is happening internally: The remaining functional liver tissue is insufficient to maintain basic metabolic function. Ammonia — normally detoxified by the liver — accumulates in the blood and reaches the brain (hepatic encephalopathy). Coagulation factors are not being produced — spontaneous bleeding occurs. The kidneys fail secondary to liver failure (hepatorenal syndrome).
What the patient feels and shows:
- Jaundice (yellowing of skin and eyes from bilirubin accumulation)
- Confusion, disorientation, agitation (hepatic encephalopathy)
- Spontaneous bleeding — from gums, nose, IV sites
- Kidney failure — reduced urine output, fluid retention
- Progressive loss of consciousness
- Without intervention: coma and death
In the 3D multi-organ model, Phase 4 shows the cascade of secondary organ failures triggered by liver collapse. The brain shown receiving toxic ammonia. The kidneys shown losing perfusion. The coagulation cascade shown breaking down. The visualization makes viscerally clear why liver failure is a systemic event — not just a liver event.
| Phase 4 Symptom | Mechanism | 3D Visual |
|---|---|---|
| Jaundice | Bilirubin accumulation from hepatocyte death | Skin and sclera shader turning yellow |
| Hepatic encephalopathy | Ammonia crossing blood-brain barrier | Ammonia particles shown reaching neurons |
| Spontaneous bleeding | Coagulation factor production failing | Clotting cascade shown breaking down |
| Kidney failure | Hepatorenal syndrome | Kidney perfusion shown declining |
| Coma | Combined toxic and metabolic brain failure | Neural activity shown collapsing |
Stage 2: Diagnostic Markers — How Doctors Track the Damage
Understanding mushroom poisoning symptoms from a medical perspective requires understanding the laboratory markers that reveal what is happening inside the liver — often before or despite what the patient is feeling.
The Key Lab Values in Amatoxin Poisoning:
ALT and AST (Liver Enzymes) Released into the bloodstream when hepatocytes rupture. In our 3D model, I rendered the ALT/AST rise as a graph overlaid on the liver visualization — flat during Phase 1, sharply rising in Phase 2, peaking dramatically in Phase 3 despite the patient feeling better.
Normal ALT: <40 IU/L Phase 2 peak: 500–2,000 IU/L Phase 3 peak: 1,000–10,000+ IU/L
PT/INR (Prothrombin Time) Measures the liver’s ability to produce clotting factors. As the liver fails, PT/INR rises — meaning blood takes longer to clot. An INR above 1.5 indicates significant liver impairment. Above 2.5 indicates severe failure.
Bilirubin Processed by liver cells — rises as hepatocytes fail, producing jaundice. Normal: <1.2 mg/dL. Severe poisoning: >10 mg/dL.
Creatinine Rises as kidney function fails in Phase 4, indicating hepatorenal syndrome onset.
| Lab Marker | Normal Range | Phase 2 | Phase 3 | Phase 4 |
|---|---|---|---|---|
| ALT | <40 IU/L | 100–500 | 1,000–10,000+ | Declining (cells exhausted) |
| AST | <40 IU/L | 100–500 | 1,000–10,000+ | Declining |
| INR | <1.2 | 1.2–1.5 | 1.5–3.0 | >3.0 (critical) |
| Bilirubin | <1.2 mg/dL | 1–3 | 3–8 | >10 (jaundice) |
| Creatinine | 0.7–1.3 mg/dL | Normal | Rising | >2.0 (kidney failure) |
Stage 3: Treatment — What Medicine Can and Cannot Do
The Treatment Arsenal:
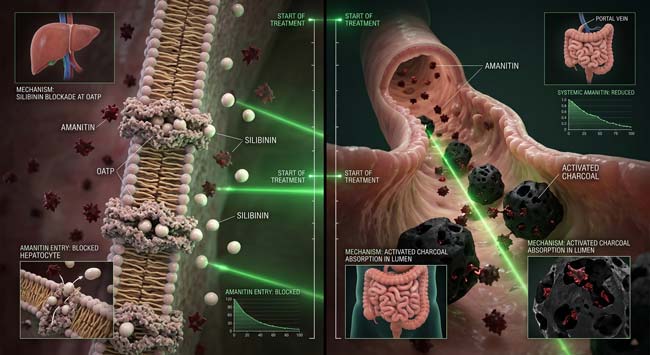
Activated Charcoal (within 1–2 hours of ingestion) Binds remaining toxin in the GI tract before absorption. In our simulation, shown as black sponge particles absorbing dark red Amanitin molecules. Highly effective if given early — ineffective once toxin has been absorbed.
Silibinin (Legalon SIL) The most specific treatment available for Amatoxin poisoning. Competitively inhibits the OATP transporters that import Alpha-Amanitin into hepatocytes — blocking further toxin entry into liver cells. In the molecular model, Silibinin particles compete with Amanitin for transporter binding sites. The earlier it is given, the more hepatocytes are saved.
N-Acetylcysteine (NAC) Replenishes glutathione — the liver’s primary antioxidant defense. Reduces oxidative damage to surviving hepatocytes. Standard treatment in most liver failure protocols.
Penicillin G Interrupts the enterohepatic recirculation of Amatoxin — preventing already-excreted toxin from being reabsorbed from the intestine.
Liver Transplant When liver failure is irreversible — indicated by severe coagulopathy, encephalopathy, and rising creatinine — emergency liver transplant is the only life-saving option. The assessment window is typically 72–96 hours from ingestion. After this window, the patient may be too unstable for transplant surgery.
| Treatment | Timing | Mechanism | Effectiveness |
|---|---|---|---|
| Activated charcoal | Within 1–2 hours | Binds GI toxin | High if early, zero if late |
| Silibinin | Within 24–48 hours | Blocks hepatocyte toxin import | High if early |
| NAC | Any phase | Antioxidant support | Moderate — supportive |
| Penicillin G | Early phases | Interrupts recirculation | Moderate |
| Liver transplant | 72–96 hour window | Replaces failed organ | Life-saving when indicated |
According to the European Association for the Study of the Liver (EASL), outcomes in Amanita phalloides poisoning are directly correlated with time to treatment — patients receiving Silibinin within 24 hours of ingestion have substantially better survival rates than those treated after 48 hours. EASL: Clinical Guidelines on Acute Liver Failure
FAQ: Mushroom Poisoning Symptoms
Q1: How do I know if I ate a toxic mushroom before symptoms appear? You often cannot know based on how you feel — this is what makes amatoxin poisoning so dangerous. If you ate any wild mushroom you are not 100% certain about, seek emergency medical care immediately regardless of how you feel. Bring a sample of the mushroom if possible — identification by a mycologist can guide treatment. Do not wait for symptoms.
Q2: Can you survive Amanita phalloides poisoning without a liver transplant? Yes — if treated aggressively early enough. Patients who receive Silibinin, NAC, and supportive care within the first 24 hours of ingestion, and whose liver damage does not progress to irreversible failure, can recover with their native liver. Survival without transplant depends entirely on how much hepatocyte loss occurred before treatment began.
Q3: Why does the False Recovery phase happen? The GI phase is driven by intestinal epithelial cell failure and inflammatory response — both of which are somewhat self-limiting as the body adapts. The liver destruction continues throughout but does not produce subjective symptoms until the functional liver mass drops below the threshold needed to maintain basic metabolism. This disconnect between subjective feeling and objective organ status is unique to hepatotoxic poisoning.
Q4: Are children more vulnerable to mushroom poisoning? Yes — significantly. The lethal dose of Alpha-Amanitin scales with body weight (estimated at 0.1mg/kg). A child weighing 20kg has a lethal threshold approximately one-quarter that of an average adult. Children are also more likely to pick and consume wild mushrooms out of curiosity. Pediatric mushroom poisoning cases require the most urgent intervention.
Q5: How long does recovery take after surviving mushroom poisoning? For mild to moderate cases, full liver function recovery typically takes 4–8 weeks as surviving hepatocytes regenerate. Severe cases requiring transplant involve the standard transplant recovery timeline — months of immunosuppression and monitoring. Some patients experience persistent liver function abnormalities for months after apparent recovery from moderate poisoning.
Conclusion: The Four Phases Are the Message
Mushroom poisoning symptoms — particularly from the most dangerous species — are not what most people imagine. There is no immediate burning or obvious alarm. There is silence, then GI distress, then apparent recovery, then organ failure.
In 3D, rendering all four phases simultaneously — the silent cellular destruction, the deceptive GI symptoms, the false recovery, and the final hepatorenal cascade — makes the complete picture visible in a way that a symptom list cannot. The body’s external experience and its internal reality are completely disconnected for the most dangerous part of the poisoning sequence.
The single most important message this simulation communicates: if you ate a wild mushroom you cannot positively identify, go to the emergency room now — not when you feel sick, not when your symptoms worsen, and definitely not when you feel better after initial symptoms resolve.
The False Recovery phase kills people who believe they have survived.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured hepatocyte death progression and lab marker rise dynamics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating liver cell translucency changes from healthy to destroyed |
| Physics Engine | Volumetric Particle System | Visualized Amanitin particles, OATP transport, and cellular death cascade |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of mushroom poisoning symptom phases |
Read more on What Happens If You Eat a Poisonous Mushroom?
Pingback: What Happens If You Eat a Poisonous Mushroom? 3D Toxin Guide