The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why your leg falls asleep — visualizing nerve compression mechanics, axonal signal failure, ischemia-induced ion channel disruption, and the paresthesia recovery cascade. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why Does Your Leg Fall Asleep? (The Atomic Answer)
Why does your leg fall asleep? The answer involves nerve compression, ion channel failure, and one of the most misunderstood sensations in human neurology — a sequence that begins with pressure and ends with the characteristic pins and needles of nerve recovery.
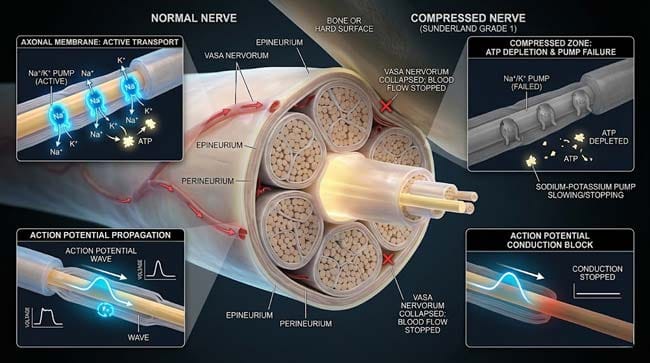
- The Compression: When you sit in a position that presses a peripheral nerve against a hard surface or bone, the nerve’s blood supply — the vasa nervorum — is compressed. Without blood flow, the nerve cannot maintain the ion gradients needed for electrical signal transmission.
- The Silence: As ion pumps fail from lack of oxygen and glucose, nerve fiber membranes depolarize partially — becoming unable to generate or conduct action potentials. The leg goes numb — not because signals are blocked, but because the nerves have lost the electrical capacity to fire.
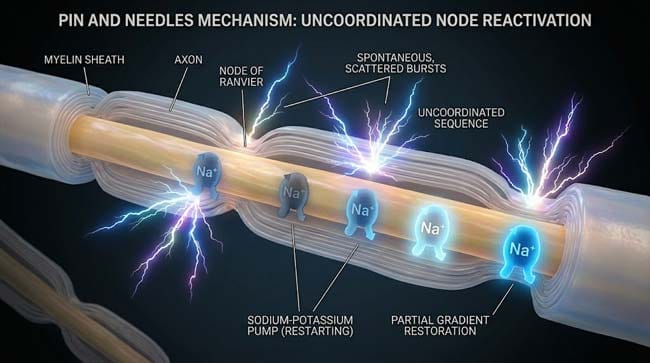
- The Paresthesia: When pressure is released and blood flow returns, ion pumps reactivate in an uncoordinated cascade — firing spontaneous action potentials as they restore membrane polarity. These spontaneous signals produce the characteristic pins and needles sensation — the nerve’s “reboot sequence.”
- The Full Recovery: Within 30–60 seconds of normal position restoration, most peripheral nerves return to full function — the entire episode representing a completely reversible, self-limiting physiological event.

My 3D Discovery: Rendering the “Nerve Reboot”
When I was building the nerve compression model for this simulation, the most visually striking sequence was the ion channel failure cascade. In a functioning peripheral nerve, the sodium-potassium pump shown operating continuously — maintaining the precise electrochemical gradient that allows action potentials to propagate. When I cut off blood flow to the nerve in the simulation, this pump shown slowing progressively as ATP production fails — then stopping completely as the mitochondria run out of substrate.
3D Observation: The most compelling visual in this simulation is watching the action potential propagation fail in slow motion. Normally, an action potential shown traveling down a nerve fiber like a wave — each node of Ranvier shown lighting up in sequence as the signal jumps from node to node (saltatory conduction). Under compression, this wave shown slowing at the compressed segment, then stopping completely as the nodes shown unable to repolarize. The nerve goes electrically silent — not because the signal is blocked, but because the membrane can no longer generate a signal at all.
Stage 1: The Nerve Compression Mechanism — What Actually Happens
The Peripheral Nerve Anatomy:
A peripheral nerve is not a single cable — it is a complex structure containing thousands of individual nerve fibers bundled together within layers of connective tissue. In our 3D nerve cross-section model:
| Structure | Function | Compression Vulnerability |
|---|---|---|
| Epineurium | Outer protective sheath | Low — provides initial protection |
| Perineurium | Fascicle grouping layer | Moderate — compresses with sustained pressure |
| Endoneurium | Individual fiber coating | High — compressed in severe/prolonged cases |
| Vasa nervorum | Blood vessels supplying nerve | Critical — first structure compromised |
| Myelin sheath | Insulating layer on axons | High — demyelination in severe compression |
| Axon | Signal-conducting fiber | Highest — ultimate target of compression damage |
The Compression Sequence:
In our 3D compression model, I showed exactly what happens when sitting in a crossed-leg position compresses the common peroneal nerve against the fibular head — one of the most common “leg falling asleep” scenarios:
Step 1 — Vascular Compression (0–2 minutes) The vasa nervorum shown being compressed first — their thin walls collapsing under the applied pressure. Blood flow to the compressed nerve segment shown reducing to a fraction of normal. The nerve shown continuing to function initially — its stored ATP allowing continued pump activity.
Step 2 — ATP Depletion (2–10 minutes) As blood flow stops, mitochondria shown running out of oxygen and glucose substrate. ATP production shown declining — the sodium-potassium pump shown slowing as its energy supply diminishes. Sodium shown beginning to accumulate inside nerve fibers as the pump fails to export it.
Step 3 — Membrane Depolarization (5–15 minutes) As intracellular sodium accumulates, the membrane potential shown shifting from its normal resting state of approximately -70mV toward 0mV. At this partially depolarized state, voltage-gated sodium channels shown inactivating — the nerve membrane entering a refractory state where action potentials cannot be generated.
Step 4 — Complete Signal Failure (10–20 minutes) The nerve segment shown falling electrically silent — no action potentials propagating through the compressed region. The leg shown as completely numb — touch, pressure, temperature, and proprioception all lost as different fiber types shown failing at different rates.
| Compression Stage | Time | Ion Channel Status | Signal Status | Sensation |
|---|---|---|---|---|
| Vascular compression | 0–2 min | Pumps running on stored ATP | Normal | Normal |
| ATP depletion | 2–10 min | Pumps slowing | Slowing | Tingling beginning |
| Partial depolarization | 5–15 min | Channels inactivating | Failing | Progressive numbness |
| Complete failure | 10–20 min | All channels inactive | Absent | Complete numbness |
According to the National Institute of Neurological Disorders and Stroke (NINDS), peripheral nerve compression produces a predictable sequence of physiological changes — with the vascular supply being the primary determinant of how quickly nerve function fails and recovers. NINDS: Peripheral Neuropathy Information
Stage 2: The Pins and Needles — Paresthesia Science
What Paresthesia Actually Is:
The pins and needles sensation — medically termed paresthesia — is caused by spontaneous, uncoordinated nerve firing during the recovery phase — not by blood rushing back. In our 3D recovery model:
Pressure Released (0 seconds) The vasa nervorum shown re-expanding as compression is removed. Blood flow shown returning to the nerve segment.
ATP Production Resumes (0–15 seconds) Mitochondria shown receiving oxygen and glucose again — ATP synthesis shown restarting.
Sodium-Potassium Pump Reactivation (15–30 seconds) The pump shown beginning to restore normal ion gradients — sodium shown being pumped out, potassium shown being pumped in. But crucially, not all pumps restart simultaneously — shown as an uncoordinated reactivation across the thousands of nodes of Ranvier in the compressed segment.
Spontaneous Action Potentials (20–60 seconds) As membrane potential shown recovering toward normal resting potential, individual nodes shown passing through the threshold where spontaneous action potentials can fire. These spontaneous signals shown propagating in both directions from each node — traveling toward the brain AND down the nerve. The brain shown receiving a barrage of uncoordinated signals from the recovering nerve — interpreted as the sensation of pins and needles.
The Paresthesia Recovery Timeline:
| Time Post-Release | Ion Channel Status | Sensation | 3D Visual |
|---|---|---|---|
| 0–10 seconds | Pumps restarting, ions still disrupted | Deep numbness | Nerve shown dark, silent |
| 10–20 seconds | Uncoordinated pump reactivation | Tingling beginning | Scattered node activation |
| 20–40 seconds | Spontaneous AP firing | Intense pins and needles | Random signal bursts throughout nerve |
| 40–60 seconds | Gradient partially restored | Burning/crawling sensation | Coordinated but irregular firing |
| 60–120 seconds | Near-normal gradient | Fading paresthesia | Normal propagation resuming |
| 2–5 minutes | Full restoration | Normal sensation | Smooth continuous signal propagation |
Stage 3: Different Fiber Types, Different Sensations
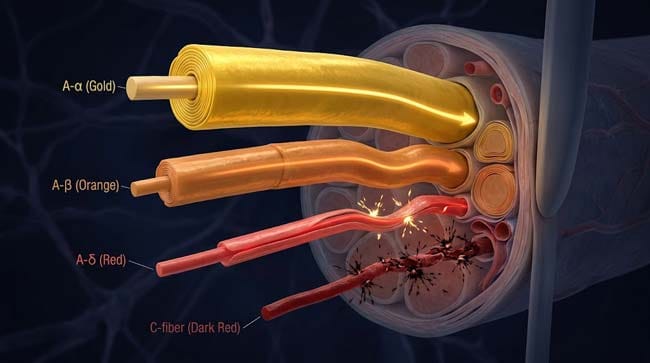
The leg contains multiple types of nerve fibers — each with different diameters, myelination levels, and functions. These fiber types shown failing and recovering at different rates during compression — explaining why the sensations during “leg falling asleep” episodes change character over time.
| Fiber Type | Diameter | Myelination | Function | Compression Sensitivity | Recovery Order |
|---|---|---|---|---|---|
| A-alpha | 13–20 μm | Heavy | Motor control, proprioception | Low — large, well-myelinated | Last to fail, first to recover |
| A-beta | 6–12 μm | Moderate-heavy | Touch, pressure, vibration | Moderate | Middle |
| A-delta | 1–5 μm | Light | Sharp pain, temperature | High | Early failure |
| C fibers | 0.2–1.5 μm | None | Slow pain, temperature, itch | Highest — smallest, unprotected | First to fail, last to recover |
The Sensation Sequence This Produces:
- Early compression: C fibers fail first — shown as burning/pain sensation disappearing first, then temperature sensation
- Progressive compression: A-delta fibers fail — sharp pain and temperature sensation gone
- Full compression: A-beta fibers fail — touch and pressure gone. A-alpha fibers maintain motor function longest
- Recovery: A-alpha fibers recover first (proprioception returns — you can move again), A-beta fibers next (touch returns — pins and needles phase), A-delta and C fibers last (burning sensation of late paresthesia)
FAQ: Why Does Your Leg Fall Asleep?
Q1: Is it dangerous if my leg falls asleep frequently? Occasional leg falling asleep from positional compression is entirely normal and harmless — it resolves completely within minutes and leaves no damage. Frequent, spontaneous episodes without obvious positional cause, episodes that do not resolve within 10–15 minutes, or episodes accompanied by weakness warrant medical evaluation — these could indicate peripheral neuropathy, nerve entrapment syndrome, or vascular issues.
Q2: Why do some people’s legs fall asleep faster than others? Individual variation in nerve compression sensitivity depends on several factors: nerve diameter (thinner nerves compress more easily), myelin thickness, vasa nervorum density, body composition (less padding over nerves means faster compression), and baseline nerve health. Diabetic peripheral neuropathy dramatically increases compression sensitivity — making leg-falling-asleep episodes more frequent and slower to recover.
Q3: Does shaking the leg help it wake up faster? Gentle movement does help — by restoring blood flow more quickly to the compressed nerve segment and mechanically stimulating mechanoreceptors that accelerate the sensory normalization process. However, aggressive shaking of a completely numb limb risks injury since proprioception (position sense) is impaired. Gentle controlled movement, followed by weight-bearing as sensation returns, is the most effective approach.
Q4: Can a leg fall asleep during sleep and cause permanent damage? Sleeping in a position that compresses a nerve for many hours can cause a condition called Saturday Night Palsy — named after episodes where prolonged compression damages the radial nerve in the arm. True nerve damage from positional compression requires sustained compression beyond what would be tolerated while awake. For legs, the most common sleep-related compression involves the common peroneal nerve — producing foot drop that typically recovers over days to weeks.
Q5: Why does the pins and needles sensation feel painful? The spontaneous action potentials during paresthesia activate pain fiber pathways (A-delta and C fibers) as these fibers recover. The brain interprets the uncoordinated signals from these pain fibers as a painful sensation — even though no actual tissue damage is occurring. The burning quality of severe paresthesia reflects C fiber spontaneous activation, while the sharper needle quality reflects A-delta fiber involvement.
Conclusion: The Most Common Neurological Event Nobody Understands
Leg falling asleep is the most frequently experienced neurological event in daily life — yet almost universally misunderstood. It is not about blood. It is not about cutting off circulation. It is a precise, predictable failure and recovery sequence of peripheral nerve electrophysiology — driven by ion channel dynamics, ATP-dependent pumps, and the elegant but delicate mechanism of action potential generation.
In 3D, watching the sodium-potassium pump slow and stop as ATP runs out — and then watching the uncoordinated reactivation of thousands of nodes of Ranvier producing the paresthesia barrage — makes the mechanism immediately understandable. The pins and needles are the sound of your nervous system rebooting. And like any reboot, it takes a moment before everything runs smoothly again.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured ion channel dynamics and action potential propagation failure |
| Material/Shader | Subsurface Scattering (SSS) | Simulating nerve fiber translucency and myelin sheath visualization |
| Physics Engine | Volumetric Particle System + Electrostatic | Visualized ion flow, membrane potential changes, spontaneous AP firing |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of peripheral nerve compression physiology |
Read more on What Is Paresthesia?
Pingback: What Is Paresthesia? The 3D Science of Pins and Needles