The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why brain freeze happens — visualizing sphenopalatine ganglion activation, rapid blood vessel dilation, and the trigeminal nerve pain cascade triggered by cold food. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why Does Brain Freeze Happen? (The Atomic Answer)
You eat ice cream too fast. Suddenly — a sharp, stabbing pain explodes behind your eyes and across your forehead. Your brain feels like it is literally freezing. But it is not.
Brain freeze is one of the most complete sensory illusions in human neurology.
- The Real Name: The medical term for brain freeze is Sphenopalatine Ganglioneuralgia (SPG neuralgia) — named after the nerve cluster at the center of the event.
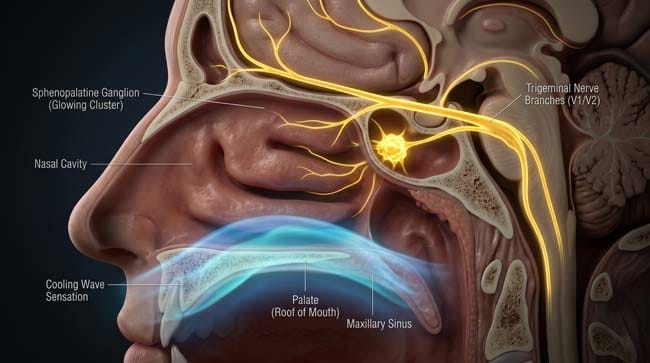
- The Trigger: Cold food or drink contacts the roof of your mouth (palate), rapidly cooling the blood vessels near the Sphenopalatine Ganglion — a nerve bundle sitting directly behind your nasal cavity.
- The Deception: Your brain interprets the sudden temperature change as a threat. The SPG fires a pain signal through the Trigeminal Nerve — the same nerve responsible for headaches — producing intense referred pain in the forehead and behind the eyes.
- The Reality: Your brain is not cold, not frozen, and not damaged. The pain is entirely a neurological alarm triggered by blood vessel behavior — not actual brain tissue temperature change.
- The Timeline: Brain freeze typically peaks within 20–30 seconds of cold contact and resolves within 30–90 seconds as blood vessels re-regulate.
My 3D Discovery: Rendering the “False Alarm” Inside Your Skull
When I was building the vascular model for this simulation, the most visually striking moment was watching the blood vessels near the Sphenopalatine Ganglion respond to cold contact. In a normal state, these vessels pulse at a steady rhythm — a calm, consistent flow of warm blood.
The moment cold food touches the palate, the vessels constrict rapidly — then dilate even faster in a rebound response. In the 3D viewport, this looks like a blood vessel suddenly going from a narrow pipe to a fully expanded tube in under two seconds. The rapid dilation is the trigger for everything that follows.
3D Observation: The most visually compelling part of this simulation is the signal pathway. The pain does not originate in the brain — it originates at the roof of the mouth, travels through the Sphenopalatine Ganglion, along the Trigeminal Nerve, and arrives at the brain’s pain processing centers as a full-intensity alarm. In the animation, you can watch this pathway light up like a fiber-optic cable — a perfect chain reaction from cold contact to forehead pain in milliseconds.
Stage 1: The Sphenopalatine Ganglion — Your Brain’s Accidental Alarm Button
The Sphenopalatine Ganglion (SPG) is a small cluster of nerve cells located in the pterygopalatine fossa — a small cavity behind your nasal passages, just above the roof of your mouth.
In normal function, the SPG manages autonomic functions in the face — controlling tear production, nasal secretions, and blood vessel dilation in the facial region. It is connected to the Trigeminal Nerve (Cranial Nerve V) — the largest and most complex cranial nerve, responsible for sensation across the entire face and head.
In our 3D anatomical model, I rendered the SPG as a dense golden node positioned directly behind the nasal cavity, with branching nerve fibers extending outward in every direction like a microscopic root system.
Why the SPG is the brain freeze trigger:
The roof of your mouth (hard palate) sits directly below the SPG’s blood vessel network. When cold food contacts this area, the temperature change is conducted rapidly through the thin palate tissue to the blood vessels immediately above — vessels that are directly monitored by the SPG.
| Anatomical Structure | 3D Visualization | Normal Function | Brain Freeze Role |
|---|---|---|---|
| Sphenopalatine Ganglion | Dense golden nerve node | Facial autonomic control | Primary alarm trigger |
| Hard Palate | Pink curved roof of mouth | Food processing surface | Cold contact point |
| Palatine Blood Vessels | Red pulsing tubes above palate | Warm blood delivery to face | Rapid temperature change site |
| Trigeminal Nerve (V2) | Golden branching cables | Facial sensation | Pain signal highway |
| Anterior Cerebral Artery | Large red vessel at brain surface | Brain blood supply | Dilation misinterpreted as threat |
According to the National Institutes of Health (NIH), Sphenopalatine Ganglioneuralgia is classified as a form of cold stimulus headache — a well-documented neurological phenomenon affecting an estimated 30–40% of the population with varying intensity. NIH: Cold Stimulus Headache

Stage 2: The Blood Vessel Cascade — What Actually Causes the Pain
This is the core of the brain freeze mechanism — and it is more complex than simply “cold = pain.”
The sequence in our 3D simulation:
Step 1 — Cold Contact (0 seconds) Ice cream contacts the hard palate. In the viewport, the temperature differential is shown as a blue cold-front spreading across the palate surface — the warm pink tissue rapidly transitioning to cool blue at the contact point.
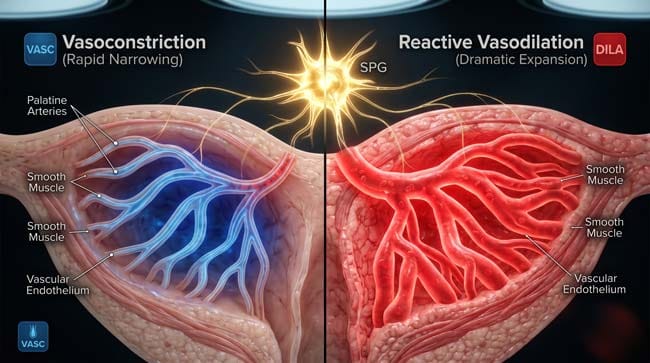
Step 2 — Vasoconstriction (0–1 second) The palatine blood vessels immediately constrict in response to cold — a standard vascular response to temperature drop. In the animation, the vessels narrow visibly, reducing blood flow.
Step 3 — Reactive Vasodilation (1–3 seconds) This is the critical moment. As the vessels constrict, the body interprets the temperature change as a potential threat to brain blood supply. The SPG triggers an immediate rebound vasodilation — the vessels expand rapidly, flooding the area with warm blood to counteract the cold.
Step 4 — SPG Activation (2–4 seconds) The sudden, rapid dilation of vessels near the SPG activates the ganglion’s sensory fibers. In the viewport, the golden SPG node suddenly pulses bright — sending signals in all directions simultaneously.
Step 5 — Trigeminal Signal Cascade (3–5 seconds) The SPG signal travels along the Maxillary Branch (V2) of the Trigeminal Nerve toward the brain. The Trigeminal Nerve, which handles sensation for the entire face and forehead, interprets the signal as a referred pain — projecting the sensation to the forehead and temples rather than the mouth where it originated.
Step 6 — Anterior Cerebral Artery Response (5–20 seconds) Simultaneously, the Anterior Cerebral Artery — which supplies blood to the frontal lobe — also dilates in response to the perceived cold threat. This arterial dilation directly beneath the frontal cortex amplifies the pain signal and explains why brain freeze feels like it is located deep inside the skull.
| Stage | Time | 3D Visual | Sensation |
|---|---|---|---|
| Cold contact | 0 sec | Blue cold-front on palate | None yet |
| Vasoconstriction | 0–1 sec | Vessels narrowing | None |
| Reactive vasodilation | 1–3 sec | Vessels rapidly expanding | Pressure building |
| SPG activation | 2–4 sec | Golden node pulsing bright | First pain wave |
| Trigeminal cascade | 3–5 sec | Signal traveling up nerve | Sharp forehead pain |
| Anterior cerebral artery dilation | 5–20 sec | Large vessel expanding at brain surface | Peak brain freeze intensity |
| Vessel re-regulation | 20–90 sec | Vessels returning to normal diameter | Pain fading |
Stage 3: Why the Pain Is Felt in the Forehead — Not the Mouth
This is the most counterintuitive aspect of brain freeze — and the most fascinating from a neurological perspective.
The cold contact happens in your mouth. The pain is felt in your forehead. Why?
Referred Pain and the Trigeminal Nerve
The Trigeminal Nerve serves three major branches:
- V1 (Ophthalmic) — forehead, scalp, upper eyelids
- V2 (Maxillary) — cheeks, upper lip, upper palate
- V3 (Mandibular) — lower jaw, lower lip, chin
When the SPG activates via the V2 branch (which covers the palate), the signal intensity overwhelms the Trigeminal system. The brain’s pain processing centers — specifically the Thalamus and Somatosensory Cortex — receive the signal but struggle to precisely locate its origin.
In our 3D brain model, this appears as a signal entering the Trigeminal nucleus, then radiating outward across multiple branches simultaneously — the brain’s pain map lighting up across the V1 territory (forehead) even though the original signal came from V2 (palate).
This is referred pain — the same mechanism that causes arm pain during a heart attack, or shoulder pain from a gallbladder problem.
Why the forehead specifically?
The forehead and temples are served by the V1 branch — the branch most sensitive to pain signals in most people. When the Trigeminal system is overwhelmed by a sudden signal, it defaults to projecting pain to its most sensitive territory.
In the 3D viewport, watching this process — a signal entering at the palate level and propagating upward to the forehead — is one of the most elegant demonstrations of referred pain mechanics in any simulation we have produced.
According to the American Migraine Foundation, brain freeze shares significant neurological pathways with migraine — which is why people who suffer from migraines tend to experience brain freeze more intensely and frequently than non-migraine sufferers. American Migraine Foundation: Brain Freeze and Migraine
FAQ: Why Does Brain Freeze Happen?
Q1: Is brain freeze dangerous? No. Brain freeze involves no actual tissue damage, no change in brain temperature, and no neurological harm. It is a pain signal produced by blood vessel behavior — not by any injury. The discomfort is real, but the threat is not. People with cardiovascular conditions should be aware that the rapid vascular changes can cause brief blood pressure fluctuations, but this is not clinically significant for healthy individuals.
Q2: Why do some people never get brain freeze? Approximately 60–70% of people experience brain freeze regularly. The remaining 30–40% either have less sensitive SPG nerve clusters, different palate vascular anatomy, or naturally slower cold conduction through palate tissue. Genetics appear to play a role in SPG sensitivity — brain freeze tendency often runs in families.
Q3: Why does brain freeze hurt behind the eyes specifically? The Ophthalmic branch (V1) of the Trigeminal Nerve covers the area around and behind the eyes. When the Trigeminal system is overwhelmed by the SPG signal, referred pain frequently localizes to the orbital region — the area around the eye socket — because this is one of the most densely innervated areas in the V1 territory.
Q4: Can you get brain freeze from things other than ice cream? Yes. Any rapid cold stimulus to the palate can trigger SPG activation — cold drinks consumed quickly, frozen foods, slushies, and even cold air inhaled rapidly through the mouth in very cold weather. The trigger is the temperature change rate at the palate, not the specific food source.
Q5: Why do people who get migraines experience worse brain freeze? Migraine sufferers have a sensitized Trigeminal system — their pain threshold for Trigeminal nerve signals is lower than average. Since brain freeze uses the same Trigeminal pathways as migraine, the signal is interpreted with greater intensity. Some researchers are studying SPG stimulation as a potential migraine treatment precisely because of this shared pathway.

Conclusion: Your Brain Is Lying to You — And It Does It Perfectly
Brain freeze is a masterclass in neurological misdirection. No ice is forming in your brain. No tissue is being damaged. No emergency is occurring. But every pain signal your nervous system can generate is firing simultaneously — because a small nerve cluster behind your nose detected a cold blood vessel and decided the situation was critical.
In 3D, rendering the complete sequence — from cold contact at the palate to the Anterior Cerebral Artery dilating beneath the frontal lobe — makes it visually clear why the sensation feels so internal and so intense. The pain pathway is real. The threat is not.
The same neurological sophistication that makes brain freeze so convincingly painful is the foundation of the entire human pain detection system — a system so precise that it can locate a threat to within millimeters, and so occasionally imprecise that it confuses an ice cream cone for a brain emergency.
Further Study & External Research
- NIH — Cold Stimulus Headache and SPG Neuralgia
- American Migraine Foundation — Brain Freeze and Migraine Connection
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured vascular dilation dynamics and nerve signal propagation |
| Material/Shader | Subsurface Scattering (SSS) | Simulating translucency of palate tissue and vessel walls |
| Physics Engine | Volumetric Particle System + Fluid Dynamics | Visualized blood flow changes and temperature propagation |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of Sphenopalatine Ganglioneuralgia |
Read more on How to Stop Brain Freeze Fast
Pingback: ow to Stop Brain Freeze Fast: The 3D Science Guide