The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore what eye discharge is — visualizing the biochemical composition of different discharge types, the immune and inflammatory mechanisms that produce abnormal discharge, and the diagnostic differences between normal sleep discharge and pathological eye conditions. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Is Eye Discharge? (The Atomic Answer)
What is eye discharge? Eye discharge — colloquially called “eye gunk,” “sleep,” “eye boogers,” or “rheum” — is the collective term for any material that accumulates at the eye’s surface and eyelid margins, whether during sleep or waking hours.
- The Normal Version: Normal eye discharge is a mixture of dried tear film components, meibomian gland secretions, shed epithelial cells, and trapped environmental debris — harmless, small in amount, and produced by every healthy eye during sleep.
- The Abnormal Version: Abnormal eye discharge — excessive, colored, or present during waking hours — indicates immune response, infection, allergy, or structural problems with the eye’s drainage or secretory systems.
- The Biochemistry: The color, consistency, and amount of eye discharge are direct diagnostic clues — reflecting the specific biological process producing the discharge. Purulent (pus-like) discharge means neutrophils. Watery clear discharge means viral response or allergic mediators. Stringy discharge means excessive mucin production.
- The Significance: Eye discharge is one of medicine’s most useful rapid diagnostic signs — experienced ophthalmologists can often make a working diagnosis from discharge characteristics alone before any examination of the eye itself.

My 3D Discovery: Rendering the “Diagnostic Rainbow”
When I was building the comprehensive eye discharge model for this simulation, the most clinically useful visualization was rendering different discharge types at the molecular level — showing why each looks the way it does and where each component comes from.
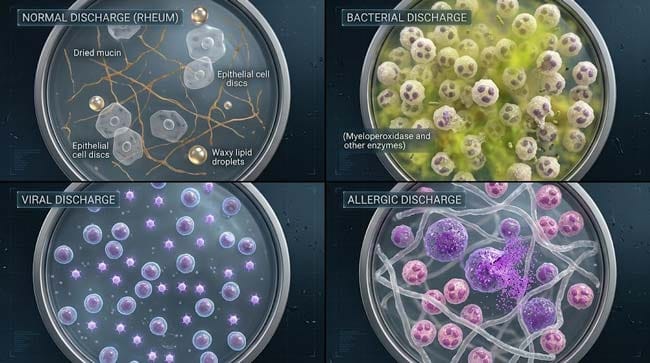
The most striking contrast was between normal morning discharge and bacterial conjunctivitis discharge. Normal discharge — shown as a small, mixed collection of dried proteins, lipid droplets, and epithelial cell remnants — looks heterogeneous and sparse at molecular scale. Bacterial discharge — shown as an overwhelming flood of neutrophils, bacterial cells, fibrin strands, and cellular debris — is visually dramatic in its density and uniformity.
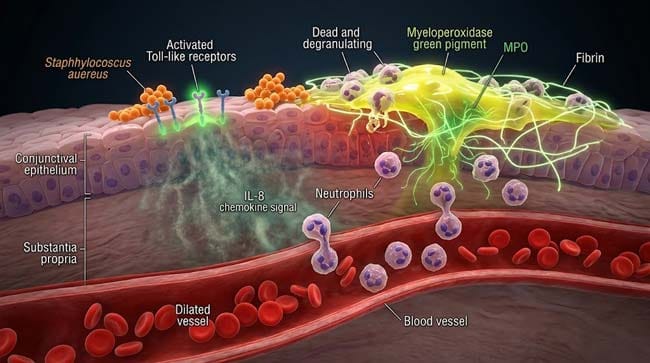
3D Observation: The most medically valuable sequence in this simulation is watching neutrophil recruitment to the conjunctival surface in bacterial conjunctivitis. Bacteria shown colonizing the conjunctival epithelium — their surface pattern recognition ligands shown activating Toll-like receptors on epithelial cells. The epithelium shown releasing IL-8 and other chemokines — shown as signal particles attracting neutrophils from the conjunctival blood vessels. Neutrophils shown arriving in massive numbers — pushing through the vessel walls and flooding the conjunctival surface. The resulting purulent discharge shown forming as accumulated dead neutrophils, bacterial debris, and fibrin — the visible evidence of the immune battle occurring at your eye surface.
Stage 1: The Complete Biochemistry — What Eye Discharge Actually Contains
The Molecular Composition by Discharge Type:
Type 1 — Normal Sleep Discharge (Rheum)
In our 3D normal discharge model, I rendered the complete composition at molecular resolution:
Dried mucins — shown as fibrous, glycoprotein strands forming the structural scaffold of the discharge. The MUC5AC mucin — produced by conjunctival goblet cells — shown as the primary structural component, its long chain molecules shown tangling and cross-linking as they desiccate overnight.
Meibomian lipid residue — shown as waxy, yellowish droplets embedded in the mucin matrix. The long-chain fatty acids and cholesterol esters from meibomian secretions shown contributing the characteristic slightly waxy consistency of dried discharge.
Desquamated epithelial cells — shown as flat, disc-shaped cells — the continuously shed superficial cells of the conjunctival epithelium. These cells shown being trapped in the mucin matrix rather than being swept into drainage by blinking.
Protein deposits — shown as amorphous deposits of concentrated lysozyme, lactoferrin, and albumin. As the aqueous component evaporates, these proteins shown precipitating out of solution — contributing the hard, crusty texture of dried morning discharge.
Commensal bacteria — shown as small numbers of Staphylococcus epidermidis and Corynebacterium species — the normal conjunctival microbiome. Present in small numbers, kept in check by the antimicrobial proteins in the tear film.
Type 2 — Bacterial Discharge
Bacterial conjunctivitis discharge shown as fundamentally different in composition:
Neutrophils (dominant component) Shown as multi-lobed white blood cells flooding the conjunctival surface. In bacterial conjunctivitis, neutrophil counts shown increasing from baseline (near zero at the conjunctival surface) to millions per milliliter of discharge. Dead and dying neutrophils shown releasing their cellular contents — the primary contributor to the yellow-green color and thick consistency.
Why Yellow-Green? The yellow-green color of purulent discharge shown coming from myeloperoxidase — a green-pigmented enzyme in neutrophil granules. When neutrophils die and release their contents, myeloperoxidase shown diffusing into the surrounding fluid — shown as green pigment particles spreading through the discharge, producing the characteristic color regardless of which bacteria caused the infection.
Bacterial cells and fragments The causative bacteria shown as either gram-positive cocci (Staphylococci, Streptococci) or gram-negative rods (Haemophilus influenzae, Pseudomonas) — their specific species often guessable from clinical context even before culture results return.
Fibrin strands Shown as fine threads forming a meshwork through the discharge — fibrin deposited from plasma proteins leaking through the inflamed, permeable conjunctival blood vessels.
Type 3 — Viral Discharge
Viral conjunctivitis (most commonly adenoviral) shown producing discharge with a completely different cellular composition:
Lymphocytes (dominant) — shown as smaller, round mononuclear cells rather than the multi-lobed neutrophils of bacterial infection. The adaptive immune response shown dominating rather than the innate neutrophil response.
Viral particles — shown as tiny icosahedral adenovirus particles in the tear film — not visible to the naked eye but shown in our molecular model as the causative agent being shed in the discharge.
Interferon proteins — shown as the antiviral signaling molecules produced by infected conjunctival cells — contributing to the watery, proteinaceous quality of viral discharge.
Type 4 — Allergic Discharge
Allergic conjunctivitis discharge shown driven by mast cell degranulation — a completely different immune mechanism:
Mast cells degranulating — shown as large, granule-filled cells in the conjunctival stroma releasing histamine, tryptase, and other mediators. This shown producing immediate vascular permeability — plasma proteins and fluid shown flooding the conjunctival surface.
Eosinophils — shown as characteristic cells of allergic inflammation, their bright red granules shown clearly in the 3D model.
Excess mucin — mast cell mediators shown stimulating goblet cells to dramatically increase mucin production — producing the characteristic stringy, ropy, mucoid discharge of allergic conjunctivitis.
| Discharge Type | Dominant Cell | Color | Consistency | Molecular Key Feature |
|---|---|---|---|---|
| Normal sleep | Epithelial cells | Clear to pale yellow | Crusty, small | Dried mucin + meibomian lipids |
| Bacterial | Neutrophils | Yellow-green | Thick, purulent | Myeloperoxidase green pigment |
| Viral | Lymphocytes | Clear, watery | Thin, watery | Interferon proteins, lymphocytes |
| Allergic | Eosinophils + mast cells | Clear | Stringy, ropy | Excess goblet cell mucin |
| Dry eye | None specific | Clear to white | Stringy, filamentous | Mucin strands without aqueous |
| Dacryocystitis | Neutrophils | Yellow-green | Purulent at puncta | Infected lacrimal sac contents |
According to the American Academy of Ophthalmology, the morphological characteristics of eye discharge — color, consistency, laterality, and time of day — provide sufficient diagnostic information to guide initial management in the majority of conjunctivitis cases, with culture and sensitivity testing reserved for cases unresponsive to empirical treatment. AAO: Conjunctivitis Preferred Practice Pattern
Stage 2: The Immune Battle — What Produces Abnormal Discharge
The Conjunctival Immune System:
The conjunctiva is one of the most immunologically active tissues in the body — it is a mucosal surface constantly exposed to environmental antigens, microorganisms, and allergens. In our 3D conjunctival immune model:
Resident immune cells shown in the normal conjunctiva:
- Mast cells — shown as large granule-containing cells throughout the conjunctival stroma — the first responders to allergens
- Dendritic cells — shown extending their processes toward the conjunctival surface — sampling the environment for antigens
- Macrophages — shown as resident phagocytes maintaining baseline immune surveillance
- IgA-producing plasma cells — shown providing the secretory IgA component of the tear film
The Bacterial Infection Cascade:
In our 3D infection cascade model, I rendered the complete sequence from bacterial contact to purulent discharge formation:
Step 1 — Bacterial Adhesion (0–2 hours) Bacteria shown arriving on the conjunctival surface — their surface adhesins shown binding to conjunctival epithelial cell receptors. The most common conjunctival pathogens shown:
- Staphylococcus aureus — shown as orange clusters — produces toxins that directly damage epithelial tight junctions
- Haemophilus influenzae — shown as small gram-negative rods — primary cause in children, often associated with otitis media
- Streptococcus pneumoniae — shown as paired cocci — produces pneumolysin shown disrupting cell membranes
- Pseudomonas aeruginosa — shown as green-pigmented rods — most serious, associated with contact lens wear
Step 2 — Epithelial Recognition (Hours 1–4) Conjunctival epithelial cells shown detecting bacterial patterns through Toll-like receptors (TLRs). TLR activation shown triggering NF-κB signaling — shown as a molecular cascade producing IL-1β, IL-6, IL-8, and TNF-α.
Step 3 — Neutrophil Recruitment (Hours 4–12) IL-8 shown acting as the primary neutrophil chemoattractant — shown as gradient of signal molecules drawing neutrophils from conjunctival blood vessels. The vessels shown dilating (shown as the redness of conjunctivitis) and becoming permeable — neutrophils shown squeezing through the vessel walls (diapedesis) and migrating to the conjunctival surface.
Step 4 — Discharge Formation (Hours 12–24) Neutrophils shown engulfing and destroying bacteria — releasing their enzymatic contents (myeloperoxidase, elastase, defensins) as they die. The accumulation of dead neutrophils, bacterial debris, fibrin, and cellular contents shown forming the characteristic purulent discharge.
The Viral Infection — A Different Battle:
Viral conjunctivitis (shown primarily as adenoviral) produces a fundamentally different immune response:
Adenovirus entry — shown as the virus binding to CAR (Coxsackie and Adenovirus Receptor) on conjunctival epithelial cells — inserting its DNA into the nucleus.
Interferon production — infected cells shown detecting viral DNA through PRRs (particularly cGAS-STING pathway) — producing Type I interferons shown as antiviral alarm signals to neighboring cells.
Natural killer cell activation — shown as NK cells arriving to destroy virus-infected cells — their perforin and granzyme attack shown killing infected epithelial cells before viral replication is complete.
Lymphocyte recruitment — shown as the adaptive immune response arriving over days — CD8+ cytotoxic T cells shown targeting infected cells, CD4+ helper T cells shown coordinating the response.
The watery, lymphocyte-dominated discharge of viral conjunctivitis shown as the relatively gentler immune response compared to the neutrophil-dominated purulent response of bacterial infection.
Stage 3: Clinical Recognition and Treatment — Reading the Discharge
The Rapid Clinical Assessment:
In our 3D clinical decision model, I showed how discharge characteristics guide immediate management:
Assessment Step 1 — Laterality:
- Unilateral → more likely bacterial (direct inoculation) or viral starting in one eye
- Bilateral from onset → more likely allergic or viral (systemic immune response)
- Bilateral sequential (one eye then other) → viral (spreading from initial infected eye)
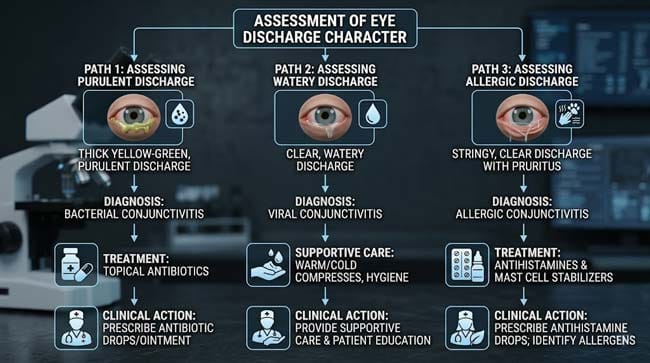
Assessment Step 2 — Discharge Character:
- Thick purulent, morning gluing → bacterial → topical antibiotics
- Watery, associated with cold → viral → supportive care, cold compresses
- Stringy with intense itch → allergic → antihistamines, mast cell stabilizers
- Small, morning only, no redness → normal → no treatment needed
Assessment Step 3 — Associated Features:
- Preauricular lymphadenopathy (swollen node in front of ear) → viral (especially adenoviral)
- Intense itch → allergic (itch is the cardinal symptom of allergy)
- Pain with eye movement → orbital involvement → urgent evaluation
- Vision change → urgent ophthalmology evaluation regardless of discharge type
Treatment by Discharge Type:
| Discharge Type | First-Line Treatment | Duration | When to Escalate |
|---|---|---|---|
| Normal morning | None — warm water rinse | N/A | If increasing amount or redness |
| Bacterial | Topical antibiotic drops/ointment | 5–7 days | No improvement in 48 hours |
| Viral | Cold compresses, lubricating drops | Self-limiting 1–3 weeks | Vision change, severe pain |
| Allergic | Topical antihistamine/mast cell stabilizer | Ongoing during exposure | Systemic symptoms, no response |
| Dry eye related | Artificial tears, treat MGD | Ongoing | Corneal involvement |
The Contact Lens Warning:
In our 3D contact lens contamination model, I showed why contact lens wearers face special risk:
Contact lenses shown creating a microenvironment between the lens and cornea — shown trapping bacteria that would normally be washed away by the tear flow. Pseudomonas aeruginosa — shown as the most dangerous contact lens-associated pathogen — shown producing a biofilm on the lens surface and producing proteases that rapidly destroy corneal tissue.
Contact lens wearers with any eye discharge should shown:
- Remove lenses immediately
- Not reinsert lenses until discharge has fully resolved
- See an eye care professional promptly — contact lens-associated infections can threaten vision within 24–48 hours
According to the Centers for Disease Control and Prevention (CDC), approximately 1 million doctor and emergency room visits annually in the United States are attributed to contact lens-related eye infections — with improper handling being the primary risk factor. CDC: Contact Lens Health
FAQ: What Is Eye Discharge?
Q1: Is it safe to remove eye discharge with my fingers? Clean hands can gently remove normal morning discharge — but touching the eye with unwashed hands introduces bacteria and increases infection risk. The safest method is using a clean, warm, damp cloth or cotton pad to gently wipe from the inner corner outward. Never rub the eye — this spreads discharge across the conjunctival surface and potentially pushes bacteria into the lacrimal system. For suspected infectious discharge, disposable tissues are preferred to prevent contaminating washcloths.
Q2: Why does eye discharge increase when you have a cold? Upper respiratory viral infections produce systemic immune activation — interferons and inflammatory mediators shown affecting the conjunctival mucosa through the bloodstream and directly from the nasal passages via the nasolacrimal duct. The nasolacrimal duct connects the eye to the nose — shown as a direct anatomical pathway for spread of nasal viruses to the conjunctiva. Rhinovirus and adenovirus shown traveling this pathway to produce the conjunctivitis commonly associated with upper respiratory infections.
Q3: Can eye discharge spread conjunctivitis to others? Yes — particularly bacterial and viral conjunctivitis. Discharge contains infectious organisms that survive on surfaces for hours. Touching your own discharge and then touching a surface shown transferring viable bacteria or viruses. The primary spread mechanism shown as: discharge on hand → handshake or shared surface → hand-to-eye contact by the new host. Hand hygiene is the most effective prevention — thorough handwashing before and after touching infected eyes dramatically reduces spread.
Q4: What causes excessive eye discharge in newborns? The most common cause is congenital nasolacrimal duct obstruction — present in approximately 6% of newborns. The nasolacrimal duct, which drains tears from the eye into the nose, shown not fully opening at birth — tears and debris shown backing up and concentrating at the medial canthus. Most cases resolve spontaneously by 12 months with gentle massage of the lacrimal sac. Persistent obstruction after 12 months may require probing of the duct under brief anesthesia.
Q5: Why do some people get more eye discharge than others? Multiple factors determine baseline discharge amount: meibomian gland function (glands producing more oil produce more discharge substrate), goblet cell density (more goblet cells = more mucin = more discharge potential), sleep duration (longer sleep = more accumulation time), environmental exposure (dust, allergens, contact lens use), and tear film stability (people with dry eye syndrome often have more discharge paradoxically, as their unstable tear film produces more mucin and cellular debris). Age also plays a role — meibomian gland function typically declines with age, paradoxically reducing the lipid layer and increasing discharge of a different character.
Conclusion: The Most Informative Fluid You Never Think About
Eye discharge is simultaneously the most ignored and most diagnostically informative fluid the human body produces. Its color tells you which immune cells are present. Its consistency tells you which molecular processes are occurring. Its timing tells you whether blinking cessation or active inflammation is responsible. Its laterality tells you whether the cause is local or systemic.
In 3D, rendering the molecular composition of each discharge type — from the heterogeneous dried proteins and lipids of normal sleep discharge to the uniform myeloperoxidase-stained neutrophil flood of bacterial infection to the stringy mucin overproduction of allergic mast cell activation — transforms what most people dismiss as “eye gunk” into a visible window into your conjunctival immune system’s current status.
The discharge is the report. Learning to read it is surprisingly useful.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured neutrophil recruitment dynamics and mast cell degranulation |
| Material/Shader | Subsurface Scattering (SSS) | Simulating conjunctival tissue and discharge fluid viscosity |
| Physics Engine | Volumetric Particle System + Fluid Dynamics | Visualized discharge composition, immune cell recruitment, myeloperoxidase diffusion |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of eye discharge biochemistry and clinical significance |
Read more on Why Do Eyes Get Stuck Shut While You Sleep?
Pingback: Why Do Eyes Get Stuck Shut While Sleeping? 3D Tear Science