The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why touching your belly button can make you dizzy — visualizing the umbilical visceral sensory nerve pathways, vagal reflex mechanics, cardiovascular response to umbilical pressure, and the neurological cascade that connects a simple touch to systemic physiological effects. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why Does Touching Your Belly Button Make You Dizzy? (The Atomic Answer)
Why does touching your belly button make you dizzy? The answer lies in a neurological reflex that most people never knew existed — connecting the umbilicus directly to the vagus nerve through visceral sensory pathways that date back to your fetal development.
- The Connection: The belly button’s inner lining is connected to the peritoneum — the membrane lining the abdominal cavity. Pressing the belly button stimulates visceral sensory nerve fibers in the peritoneum and surrounding structures that feed directly into the vagus nerve and spinal cord sensory pathways.
- The Reflex: This stimulation triggers the vasovagal reflex — a cascade of autonomic responses including decreased heart rate (bradycardia), decreased blood pressure (hypotension), and peripheral vasodilation — that can produce dizziness, nausea, and in extreme cases, fainting.
- The Urge: Many people also experience an urge to urinate when pressing the belly button — because the visceral nerve pathways from the umbilical region overlap with those from the bladder, creating referred sensations between these two structures.
- The Anatomy: This is not a myth — it is documented neuroanatomy. The umbilicus and its surrounding structures contain a dense network of visceral afferent nerve fibers with direct connections to autonomic control centers.

My 3D Discovery: Rendering the “Hidden Reflex”
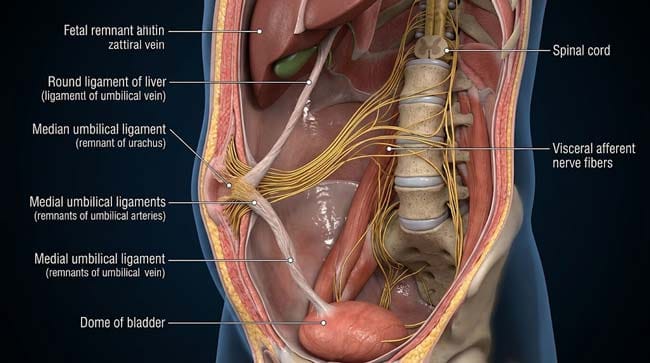
When I was building the umbilical nerve pathway model for this simulation, the most visually striking element was the density of sensory innervation in what appears to be a simple scar. In the 3D viewport, the umbilicus shown as anatomically much more complex than its exterior appearance suggests — a concentrated convergence point of visceral sensory nerve fibers from the peritoneum, the umbilical remnants (the obliterated umbilical arteries, umbilical vein — now the round ligament of the liver, and the urachus), and the anterior abdominal wall.
When I traced these nerve fibers centrally, they shown converging on the T9–T10 spinal cord segments and the dorsal vagal complex — the same autonomic control centers that regulate heart rate, blood pressure, and gastrointestinal function.
3D Observation: The most neurologically surprising visualization in this simulation is watching the cardiovascular response to belly button stimulation in real time. A single press of the umbilicus shown activating visceral afferent fibers — shown as a signal traveling up the spinal cord to the nucleus tractus solitarius in the brainstem. From there, shown as an efferent vagal signal traveling down to the heart — the SA node shown slowing its firing rate within 3–5 seconds of stimulation. Blood pressure shown dropping as peripheral vessels shown dilating. The person shown experiencing the characteristic lightheadedness of sudden blood pressure reduction — all from pressing a button that looks like a simple navel.
Stage 1: The Anatomy — Why the Belly Button Is Neurologically Special
The Umbilicus — More Than a Scar:
Most people think of the belly button as simply the remnant of where the umbilical cord attached. In reality, the umbilical region contains the remnants of several fetal structures that, while no longer functional as conduits, have left behind a concentration of nerve fibers and fascial structures that make this area neurologically unique.
The Fetal Structures That Become the Umbilical Anatomy:
In our 3D fetal anatomy model, I showed what the umbilical cord contained during fetal development:
- Two umbilical arteries — carrying deoxygenated blood from the fetus to the placenta. After birth, shown obliterating to become the medial umbilical ligaments — fibrous cords running from the umbilicus to the bladder
- One umbilical vein — carrying oxygenated blood from the placenta to the fetus. After birth, shown becoming the round ligament of the liver — running from the umbilicus to the liver
- The urachus — a canal connecting the fetal bladder to the umbilicus. After birth, shown obliterating to become the median umbilical ligament — running from the umbilicus directly to the apex of the bladder
The Critical Anatomical Connections:
These obliterated structures shown maintaining their fascial and neural connections to their original organs — creating anatomical pathways from the umbilicus to:
- The bladder (via the median umbilical ligament / obliterated urachus)
- The liver (via the round ligament)
- The peritoneum (the visceral lining covering all abdominal organs)
The nerve fibers serving these structures shown sharing spinal cord segments — creating the viscero-visceral reflex pathways that explain why umbilical stimulation produces effects felt in distant organs.
The Peritoneal Connection:
The most important neurological connection of the umbilicus is to the peritoneum — the sensitive membrane lining the entire abdominal cavity. The parietal peritoneum (lining the abdominal wall) shown densely innervated by spinal somatic and visceral afferent fibers at the T9–T10 level.
Pressing the belly button shown transmitting pressure to the underlying peritoneum — activating these visceral afferent fibers in the same way that peritoneal irritation from any cause (appendicitis, peritonitis) activates them.
| Umbilical Structure | Fetal Function | Adult Remnant | Neural Connection |
|---|---|---|---|
| Umbilical arteries (x2) | Fetal circulation to placenta | Medial umbilical ligaments | Connects to bladder nerve territory |
| Umbilical vein | Oxygenated blood from placenta | Round ligament of liver | Connects to hepatic nerve territory |
| Urachus | Bladder-umbilicus canal | Median umbilical ligament | Direct anatomical link to bladder |
| Peritoneum | Abdominal lining (continuous) | Same — unchanged | T9–T10 visceral afferents — vagal input |
| Umbilical ring | Cord passage point | Fibromuscular ring | Dense mechanoreceptor concentration |
According to the Journal of Anatomy, the umbilical region contains one of the highest concentrations of visceral afferent nerve fibers in the anterior abdominal wall — with convergence of inputs from multiple organ territories explaining the range of referred sensations produced by umbilical stimulation. Journal of Anatomy: Visceral Afferent Innervation of the Anterior Abdominal Wall

Stage 2: The Vasovagal Reflex — How Belly Button Touch Causes Dizziness
The Complete Reflex Pathway:
In our 3D reflex pathway model, I rendered the complete neurological cascade from belly button touch to dizziness:
Step 1 — Mechanoreceptor Activation (0 seconds) Pressure on the umbilicus shown transmitting through the abdominal wall to the peritoneum — activating mechanoreceptors and visceral afferent C fibers in the peritoneal tissue. These receptors shown responding to both pressure and stretch — shown activating within milliseconds of finger pressure.
Step 2 — Afferent Signal Transmission (0–0.5 seconds) Visceral afferent signals shown traveling along two pathways simultaneously:
- Spinal pathway: Signals shown entering the spinal cord at T9–T10 — traveling up the spinothalamic tract to the thalamus and hypothalamus
- Vagal pathway: Some afferent signals shown traveling via the vagus nerve directly to the nucleus tractus solitarius (NTS) in the brainstem
Step 3 — Brainstem Processing (0.5–2 seconds) The NTS shown receiving the visceral afferent input — shown as the primary integrating center for cardiovascular and autonomic responses. The NTS shown activating the dorsal motor nucleus of the vagus (DMV) — the source of vagal efferent output to the heart and abdominal organs.
Step 4 — Cardiovascular Response (2–5 seconds) The efferent vagal signal shown traveling to the sinoatrial (SA) node in the heart — shown as acetylcholine release slowing the pacemaker’s firing rate. Simultaneously, the vasomotor center shown reducing sympathetic tone to peripheral blood vessels — shown as vessels dilating throughout the body.
The combined effect: heart rate decreasing (bradycardia) and blood pressure dropping (hypotension) — shown in the cardiovascular model as blood pressure gauge reading dropping within seconds of stimulation.
Step 5 — Cerebral Perfusion Reduction (3–8 seconds) With lower blood pressure and slower heart rate, cerebral blood flow shown decreasing transiently. The brain shown receiving less blood — shown as cerebral perfusion pressure dropping. The person shown experiencing the characteristic symptoms of reduced cerebral perfusion: lightheadedness, dizziness, visual darkening, and nausea.
The Bladder Urge Connection:
The urge to urinate that many people experience when pressing the belly button shown arising from viscero-visceral cross-excitation — a well-documented phenomenon where stimulation of one visceral organ’s afferent pathway shown exciting the afferent pathways of anatomically adjacent organs.
In the 3D model, I showed the specific pathway:
The median umbilical ligament (obliterated urachus) shown running directly from the umbilicus to the bladder dome. Pressing the umbilicus shown transmitting mechanical force along this ligament — shown stimulating bladder wall mechanoreceptors. Simultaneously, shared T9–T10 visceral afferent fibers shown conducting signals from both the umbilical peritoneum and the bladder — shown producing referred sensation as if the bladder were being compressed.
The brain shown interpreting this visceral signal convergence as a need to urinate — even though the bladder itself contains no more urine than before.
| Reflex Step | Time | Neural Structure | 3D Visualization | Effect |
|---|---|---|---|---|
| Mechanoreceptor activation | 0 sec | Peritoneal C fibers | Pressure shown activating fiber endings | None perceived yet |
| Afferent signal | 0–0.5 sec | T9–T10 and vagal afferents | Signal pulse shown ascending | Slight awareness |
| NTS processing | 0.5–2 sec | Brainstem NTS | Signal shown arriving at dorsal vagal complex | Processing |
| SA node slowing | 2–5 sec | Vagal efferent to heart | Heart rate shown decreasing | Mild palpitation sense |
| Blood pressure drop | 3–6 sec | Vasomotor center → vessels | Peripheral vessels shown dilating | Lightheadedness |
| Cerebral perfusion reduction | 3–8 sec | Cerebral vessels | Brain perfusion shown decreasing | Dizziness, nausea |
Stage 3: Individual Variation — Why Some People Feel More Than Others
Why the Response Varies:
Not everyone who touches their belly button experiences dizziness. The intensity of the vasovagal response shown depending on several factors:
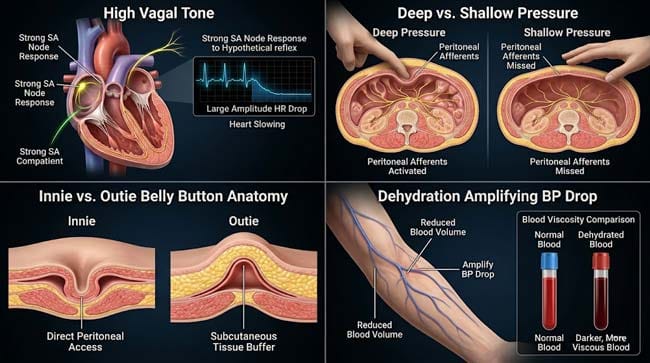
Vagal Tone: Individuals with naturally high vagal tone (athletes, highly fit individuals, people who practice meditation) shown having more pronounced heart rate responses to vagal stimulation — because their cardiovascular system is more responsive to vagal input. Paradoxically, high vagal tone is generally healthy but can make vasovagal responses more pronounced.
Depth and Pressure of Stimulation: Shallow surface pressure shown activating mainly cutaneous mechanoreceptors — producing minimal visceral response. Deep pressure directed toward the peritoneum shown dramatically more effective at activating the visceral afferents responsible for the vasovagal cascade. This is why most people need to press relatively firmly toward the peritoneal lining rather than simply touching the skin surface.
Umbilical Anatomy: People with innie belly buttons (umbilical recesses) shown having the peritoneum more accessible to pressure — shown as the umbilical recess directing pressure more efficiently toward the underlying peritoneum. People with outie belly buttons (umbilical protrusions) have more subcutaneous tissue between the skin and peritoneum — shown partially attenuating the pressure transmission.
Existing Autonomic Nervous System State: The vasovagal response shown more pronounced when the person is:
- Dehydrated (reduced blood volume amplifies blood pressure drop)
- Warm (peripheral vasodilation already partially occurring)
- Anxious or in pain (sensitized autonomic responses)
- Standing (gravity effects amplify any blood pressure reduction)
The Extreme Cases — Syncope:
In rare cases, particularly in individuals with very high vagal tone or those pressing deeply while in a sensitized autonomic state, the vasovagal response shown sufficient to produce syncope (fainting). In the 3D model:
- Heart rate shown dropping from 70 to below 40 bpm
- Blood pressure shown falling from 120/80 to below 80/50 mmHg
- Cerebral perfusion shown falling below the threshold required for consciousness
- Person shown losing postural tone and collapsing
This extreme outcome shown as rare — but it represents the same mechanism (vasovagal syncope) that causes some people to faint from pain, fear, or blood draws. The belly button simply happens to be an unusually effective trigger for this reflex in susceptible individuals.
FAQ: Why Does Touching Your Belly Button Make You Dizzy?
Q1: Is it safe to press your belly button? For healthy adults, casual touching of the belly button is completely safe. The vasovagal response produced is typically mild — slight lightheadedness that resolves within seconds of stopping stimulation. The concern arises with sustained deep pressure in standing individuals with high vagal tone — which can theoretically produce syncope. If you have a history of vasovagal syncope or fainting episodes, avoid deep umbilical pressure while standing, particularly when dehydrated or in a warm environment.
Q2: Why do some people feel like they need to pee when touching their belly button? This is the viscero-visceral cross-excitation described in Stage 2. The median umbilical ligament (obliterated urachus) creates a direct anatomical connection from the umbilicus to the bladder dome. Pressing the belly button shown transmitting mechanical stimulus along this ligament to the bladder wall, and shared T9–T10 visceral afferent fibers shown conducting convergent signals that the brain interprets as a bladder-filling sensation. This is entirely normal and does not indicate any pathology.
Q3: Does everyone experience this reflex or just some people? The neuroanatomy is present in everyone — all humans have the peritoneal visceral afferents and the vagal reflex pathway. However, the threshold and intensity of the response varies dramatically. People with higher vagal tone show more pronounced responses. People who rarely touch their belly button may have more sensitive responses than those who do so regularly. Factors like hydration, posture, and autonomic state at the time of stimulation all affect response intensity.
Q4: Can belly button stimulation be medically useful? The vagus nerve has become an important therapeutic target for conditions including epilepsy, depression, inflammatory diseases, and heart rhythm disorders. While belly button stimulation is not a standard therapeutic technique, the broader principle — that visceral afferent stimulation can activate the vagal system — underlies vagus nerve stimulation (VNS) therapy. VNS devices implanted near the vagus nerve are FDA-approved for epilepsy and treatment-resistant depression, producing effects through the same brainstem nuclei activated by umbilical stimulation.
Q5: Is it possible to permanently damage anything by pressing the belly button? In healthy adults with intact abdominal walls, pressing the belly button cannot cause internal organ damage — the peritoneum and underlying organs are well protected by the abdominal muscle layers. The one anatomical concern is umbilical hernia — a weakness in the abdominal wall at the umbilical ring through which abdominal contents can protrude. People with umbilical hernias should avoid deep sustained pressure on the belly button, as this can worsen the hernia or compress herniated contents.
Conclusion: The Body’s Most Surprising Reflex Button
The belly button is the only structure on the human body that simultaneously connects to the liver, the bladder, the peritoneum, and the vagus nerve — a unique anatomical nexus created by fetal development and maintained by the persistence of obliterated fetal structures and their associated nerve pathways.
In 3D, rendering the complete reflex cascade — from peritoneal mechanoreceptor activation through vagal brainstem processing to SA node slowing and cerebral perfusion reduction — makes immediately clear why what appears to be a simple touch produces systemic physiological effects. The belly button is not just a scar. It is a reflex button with direct access to the autonomic nervous system.
Press gently. Sit down first.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured visceral afferent signal dynamics and cardiovascular vasovagal response |
| Material/Shader | Subsurface Scattering (SSS) | Simulating peritoneal tissue and vagal nerve pathway visualization |
| Physics Engine | Volumetric Particle System + Fluid Dynamics | Visualized nerve signal propagation, heart rate slowing, blood pressure drop |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of umbilical vasovagal reflex neuroanatomy |
Read more on Belly Button Vagus Nerve Reflex
Pingback: Belly Button Vagus Nerve Reflex: The 3D Science Explained