The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore why eyes get stuck shut while sleeping — visualizing tear film composition, meibomian gland secretion, sleep-phase eyelid immobility, and the biochemical process by which tear components concentrate and solidify in the medial canthus during sleep. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: Why Do Eyes Get Stuck Shut While Sleeping? (The Atomic Answer)
Why do eyes get stuck shut while sleeping? The answer lies in what tears are actually made of, what happens when blinking stops for 7–8 hours, and where everything accumulates.
- The Tear Film: Your tears are not simple water — they are a complex three-layer fluid containing oils, water, proteins, mucins, lysozyme, immunoglobulins, and cellular debris. During waking hours, blinking spreads this film continuously and sweeps debris toward the lacrimal drainage system.
- The Blinking Stop: During sleep, blinking ceases entirely. The tear film shown no longer being replenished or swept — its components shown concentrating progressively as the aqueous layer evaporates.
- The Accumulation: The medial canthus (inner corner of the eye) is the natural drainage point where tears collect before entering the nasolacrimal duct. During sleep, this corner shown collecting all tear film debris — dead epithelial cells, mucin strands, oil droplets, and proteins — in one location.
- The Solidification: As the aqueous component evaporates overnight, the concentrated debris shown drying and hardening — producing the characteristic crusty or sticky discharge that can glue the eyelids together by morning.

My 3D Discovery: Rendering the “Overnight Chemistry”
When I was building the tear film concentration model for this simulation, the most visually striking sequence was the time-lapse of tear film transformation overnight. During waking hours, the tear film shown as a dynamic, constantly renewed three-layer system — the lipid layer glistening on the surface, the aqueous layer beneath maintaining hydration, the mucin layer anchoring everything to the corneal surface.
As sleep begins and blinking stops, the time-lapse shown a progressive transformation. The lipid layer shown concentrating as blinking no longer spreads it. The aqueous layer shown reducing in volume as evaporation continues without replenishment. The mucin layer shown accumulating loose epithelial cells and debris. Over 8 hours, this concentrated mixture shown migrating to the medial canthus — the natural drainage point — where it slowly desiccates into the morning eye discharge.
3D Observation: The most visually compelling moment in this simulation is the meibomian gland secretion accumulation. During waking hours, meibomian gland secretions (the lipid component of tears) shown being continuously spread across the eye surface by blinking — maintaining the lipid layer that prevents aqueous evaporation. During sleep, these glands shown continuing to produce secretion while blinking has stopped — shown accumulating at the eyelid margins. By morning, this unspread lipid secretion shown as a visible waxy accumulation at the inner corner — a significant component of morning eye discharge.
Stage 1: The Tear Film — What Your Eyes Are Made Of
The Three-Layer Tear Film:
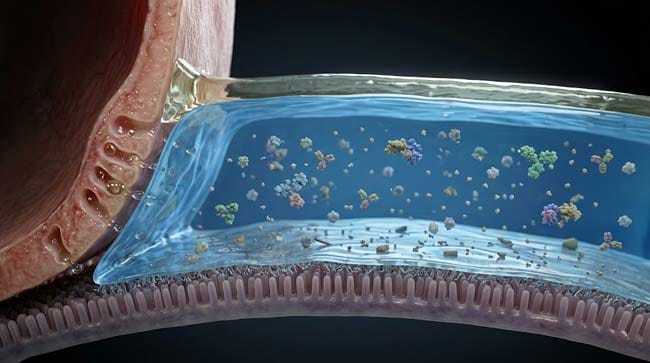
The tear film covering your cornea and conjunctiva is one of the most complex biological fluids produced by the human body — a precisely engineered three-layer structure that performs multiple simultaneous functions.
In our 3D tear film model, I rendered each layer at molecular resolution:
Layer 1 — Lipid Layer (Outermost) Produced by the meibomian glands — specialized sebaceous glands located in the upper and lower eyelid margins. Approximately 0.1 micrometers thick — shown as a thin oily film floating on the aqueous layer.
Functions shown:
- Prevents evaporation — the lipid layer shown reducing aqueous evaporation by up to 95% compared to an unprotected water surface
- Provides optical clarity — shown as a smooth optical surface for incoming light
- Lubricates the eyelid — reduces friction during blinking
Layer 2 — Aqueous Layer (Middle) Produced by the lacrimal glands — shown as large glands in the superolateral orbit. Approximately 7 micrometers thick — the thickest layer, containing most of the tear volume.
Contents shown in 3D model:
- Water — primary component (~98%)
- Lysozyme — enzyme shown destroying bacterial cell walls (antimicrobial)
- Lactoferrin — iron-binding protein shown starving bacteria of iron
- Immunoglobulin A (IgA) — antibody shown providing immune defense
- Electrolytes — sodium, potassium, chloride, bicarbonate for osmotic balance
- Growth factors — EGF and other factors shown supporting corneal cell renewal
Layer 3 — Mucin Layer (Innermost) Produced by goblet cells in the conjunctival epithelium. Approximately 0.02–0.05 micrometers thick — shown anchoring the aqueous layer to the hydrophobic corneal surface.
Functions:
- Anchors tear film — shown converting the hydrophobic corneal surface to hydrophilic, allowing aqueous layer adhesion
- Traps debris — shown capturing dead cells, bacteria, and environmental particles
- Lubricates — reduces friction between eyelids and eye surface
| Tear Film Layer | Producer | Thickness | Primary Components | Sleep Effect |
|---|---|---|---|---|
| Lipid | Meibomian glands | 0.1 μm | Cholesterol esters, phospholipids, waxes | Accumulates at lid margin — not spread |
| Aqueous | Lacrimal glands | ~7 μm | Water, proteins, electrolytes, antibodies | Evaporates and concentrates |
| Mucin | Goblet cells | 0.02–0.05 μm | Mucins, trapped debris | Accumulates with debris |
According to the American Academy of Ophthalmology, the tear film is replaced approximately every 10–30 seconds during normal waking blinking — meaning it is completely renewed hundreds of times per day. During 8 hours of sleep without blinking, this renewal ceases entirely, allowing concentration and accumulation to occur. AAO: Tear Film and Dry Eye Disease
Stage 2: What Happens During Sleep — The 8-Hour Accumulation
The Blinking Stop:
Normal blinking rate during waking hours: approximately 15–20 blinks per minute. During focused tasks (reading, screen use): 3–8 blinks per minute. During sleep: zero blinks.
In our 3D blinking mechanics model, each blink shown performing four simultaneous functions:
- Spreading the tear film from the meibomian gland reservoirs at the lid margins
- Sweeping debris and dead cells toward the medial canthus for drainage
- Pumping tears into the nasolacrimal duct through mechanical compression of the lacrimal sac
- Renewing the aqueous layer from the lacrimal gland
When blinking stops at sleep onset, all four functions cease simultaneously — shown in the animation as the dynamic tear film renewal system shown coming to a complete stop.
The Concentration Process:
During sleep, three simultaneous processes shown concentrating tear components:
Evaporation: The lipid layer, no longer being spread by blinking, shown developing gaps. Through these gaps, aqueous layer shown evaporating — the tear film volume shown decreasing progressively over the sleep period.
Protein Concentration: As aqueous volume decreases, the protein concentration shown rising. Lysozyme, lactoferrin, and mucins shown becoming increasingly concentrated — shown as their molecular density increasing in the remaining tear fluid.
Debris Accumulation: The conjunctival and corneal epithelium continuously shed dead cells — shown as desquamated epithelial cells joining the tear film. Without blinking to sweep these toward drainage, they shown accumulating in the tear film.
The Medial Canthus Collection:
The medial canthus (inner corner of the eye) is the anatomical location where tears collect before draining into the lacrimal puncta (the tiny drainage openings) and down the nasolacrimal duct into the nose.
During sleep, the medial canthus shown as a collection point for all accumulated material — gravity shown drawing concentrated tear components, dead cells, meibomian secretions, and debris to this lowest point of the eye’s drainage system.
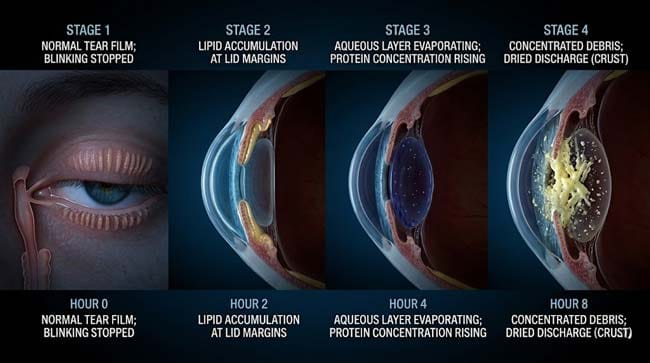
Over 8 hours:
- Hours 0–2: Soft, mucoid material beginning to collect in the medial canthus
- Hours 2–4: Increasing protein concentration and debris accumulation
- Hours 4–6: Material shown beginning to desiccate as overnight evaporation continues
- Hours 6–8: Concentrated protein-mucin-lipid composite shown hardening into the characteristic morning eye discharge
The Composition of Morning Eye Discharge:
In our 3D composition model, I analyzed what morning eye discharge actually contains:
| Component | Source | % of Discharge | 3D Visualization |
|---|---|---|---|
| Dried mucin | Goblet cells, trapped debris | 30–40% | Stringy fibrous matrix |
| Meibomian lipids | Eyelid gland secretions | 20–30% | Waxy yellowish material |
| Dead epithelial cells | Conjunctival desquamation | 15–25% | Pale flat disc-shaped particles |
| Proteins (lysozyme, etc.) | Lacrimal gland secretions | 10–15% | Concentrated protein film |
| Bacteria (commensal) | Normal conjunctival microbiome | 5–10% | Tiny rod and sphere shaped cells |
| Dried aqueous residue | Evaporated tear film water | Remainder | Crystallized salt deposits |
Stage 3: Normal vs. Abnormal — When Eye Discharge Signals a Problem
Normal Morning Eye Discharge:
The key characteristics of normal morning eye discharge:
- Amount: Small — a few small crusty deposits in the medial canthus
- Color: Clear to pale yellow or light green (the green reflects the high lysozyme content — not infection)
- Consistency: Crusty or slightly sticky — becomes hard when dried
- Location: Medial canthus (inner corner) only
- Symptoms: No associated eye pain, redness, or vision change
- Resolution: Easily removed with warm water
Abnormal Eye Discharge — When to Seek Medical Care:
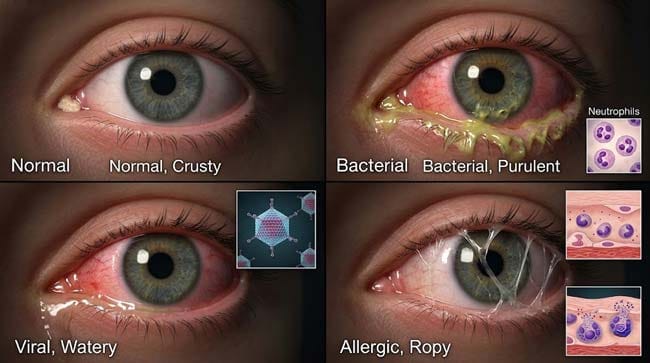
In our 3D pathology model, I showed how different types of abnormal discharge indicate different conditions:
Bacterial Conjunctivitis: Shown as thick, yellow-green, copious discharge — described as “purulent.” Bacteria shown overwhelming the eye’s normal antimicrobial defenses — neutrophils shown flooding the conjunctival tissue. Discharge shown produced throughout the day, not just in the morning. Characteristic feature: eyes shown glued shut so completely in the morning that they require warm water soaking to open.
Viral Conjunctivitis: Shown as watery, clear discharge — less thick than bacterial. Shown often associated with a respiratory infection. Highly contagious — shown as adenovirus particles spreading easily from eye contact to hands to surfaces.
Allergic Conjunctivitis: Shown as clear, stringy, ropy discharge — the characteristic mucin-rich discharge of mast cell degranulation. Shown associated with significant itching and bilateral involvement.
Dacryocystitis (Lacrimal Sac Infection): Shown as discharge specifically from the medial canthus with associated swelling and redness of the lacrimal sac region. The nasolacrimal drainage system shown obstructed and infected.
| Discharge Type | Color | Consistency | Amount | Likely Cause | Action Needed |
|---|---|---|---|---|---|
| Clear/pale crust | Clear to pale yellow | Crusty — morning only | Small | Normal — sleep discharge | None |
| Thick yellow-green | Yellow-green | Thick, purulent | Moderate-large | Bacterial conjunctivitis | See doctor |
| Watery, clear | Clear | Watery | Moderate | Viral conjunctivitis | Usually self-limiting |
| Stringy, clear | Clear | Ropy, mucoid | Variable | Allergic conjunctivitis | Antihistamines; see doctor |
| Medial canthus + swelling | Yellow | Purulent | Small-moderate | Dacryocystitis | Urgent — see doctor |
| Any discharge + vision change | Any | Any | Any | Multiple — urgent | Emergency evaluation |
FAQ: Why Do Eyes Get Stuck Shut While Sleeping?
Q1: Is it normal for eyes to be stuck shut every morning? Yes — small amounts of morning eye discharge are completely normal for virtually everyone. The amount varies between individuals based on meibomian gland activity, sleep duration, and individual tear film composition. People who sleep longer or with their eyes slightly open (lagophthalmos) tend to have more morning discharge. The only concern is if the discharge is large in amount, purulent (thick yellow-green), present during the day, or associated with eye redness, pain, or vision changes.
Q2: Why do babies have more eye discharge than adults? Newborns and infants frequently have more morning eye discharge for two reasons: their nasolacrimal ducts are often not fully open at birth (present in approximately 6% of newborns as congenital nasolacrimal duct obstruction), preventing normal tear drainage, and their conjunctival immune system is still maturing. Most congenital nasolacrimal duct obstruction resolves spontaneously by 12 months with gentle massage of the lacrimal sac.
Q3: Does sleeping with eyes open cause more discharge? Yes significantly. Approximately 20% of people sleep with their eyes partially open — a condition called nocturnal lagophthalmos. With the eyelids not fully closed, the exposed corneal and conjunctival surface shown experiencing dramatically increased evaporation — concentrating tear components faster and drying the eye surface. These individuals typically wake with significantly more discharge, more eye discomfort, and are at higher risk for corneal dryness and exposure keratopathy.
Q4: Why is morning eye discharge sometimes green even without infection? The green color of normal morning eye discharge comes primarily from lysozyme — the antimicrobial enzyme that is one of the most concentrated proteins in tears. Lysozyme’s molecular structure reflects light in the green-yellow range at the concentrations achieved in dried discharge. This is distinct from the thick, copious, bright yellow-green discharge of bacterial infection. Normal discharge is small, easily removed, and produces no discomfort — if in doubt, medical evaluation is appropriate.
Q5: Does not wearing eye makeup reduce morning eye discharge? Yes — eye makeup, particularly mascara and eyeliner, can clog meibomian glands if not thoroughly removed. Clogged meibomian glands (meibomian gland dysfunction, MGD) reduce the quality and quantity of the lipid layer — increasing aqueous evaporation and producing a cycle of tear film instability. People with MGD typically have more symptomatic dry eye and more morning discharge. Thorough eye makeup removal and lid hygiene (warm compresses, gentle lid massage) significantly reduces this risk.
Conclusion: The Overnight Chemistry of Your Eyes
Morning eye discharge is not a sign that something is wrong — it is a record of what your tear film does during 8 hours without blinking. The concentration of proteins, the accumulation of meibomian secretions, the collection of shed epithelial cells, and the overnight desiccation of everything at the medial canthus produces a small, harmless composite of every component your tear film contains.
In 3D, watching the tear film transform overnight — from a dynamic, constantly renewed three-layer protective system to a concentrated, evaporating, debris-laden fluid slowly desiccating at the inner corner of the eye — makes the morning experience immediately understandable.
Your eyes were protecting themselves all night. The discharge is the evidence.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured tear film concentration dynamics and meibomian secretion accumulation |
| Material/Shader | Subsurface Scattering (SSS) + Fluid Simulation | Simulating tear film layer dynamics and discharge desiccation |
| Physics Engine | Fluid Dynamics + Particle System | Visualized evaporation, protein concentration, debris accumulation |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of sleep-phase tear film biochemistry |
Read more on What Is Eye Discharge?
Pingback: What Is Eye Discharge? The 3D Biochemistry of Eye Gunk