The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore what paresthesia is — visualizing the neurological mechanisms behind acute and chronic pins and needles, the difference between positional and pathological paresthesia, and when the tingling sensation signals a serious underlying condition. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Is Paresthesia? (The Atomic Answer)
What is paresthesia? Paresthesia is any abnormal skin sensation — tingling, burning, numbness, prickling, or the classic pins and needles feeling — produced by inappropriate or spontaneous nerve firing without a corresponding external stimulus.
- The Definition: Paresthesia (from Greek: para = abnormal, aisthesia = sensation) describes any sensation produced by the nervous system that does not correspond to an actual external stimulus. The nerve is firing — but there is nothing touching you.
- The Two Types: Transient paresthesia — the familiar pins and needles from a compressed limb — resolves completely when the cause is removed. Chronic paresthesia — persistent tingling, numbness, or burning — indicates an ongoing neurological problem requiring medical evaluation.
- The Mechanism: Both types share the same fundamental cause — nerve fibers firing spontaneous action potentials without being triggered by a real sensory input. The difference is what is causing the spontaneous firing: temporary ion gradient disruption (transient) versus structural nerve damage, demyelination, or metabolic disease (chronic).
- The Importance: Chronic paresthesia is a cardinal symptom of over 30 distinct medical conditions — ranging from vitamin deficiencies and diabetes to multiple sclerosis and spinal cord compression. Persistent unexplained paresthesia always warrants medical evaluation.
My 3D Discovery: Rendering “Noise in the Signal”
When I was building the paresthesia visualization model for this simulation, the most conceptually interesting challenge was showing the difference between normal sensation and paresthesia using the same neurological hardware. In normal sensation, a touch receptor fires an action potential in response to an actual touch — the signal is real, appropriate, and proportional.
In paresthesia, the nerve shown firing the same type of action potential — but without any touch triggering it. The brain receives the signal and interprets it as sensation — because it has no way to distinguish between legitimate sensory input and spontaneous neural noise. The sensation feels real because, at the neurological level, it is real — a genuine action potential reaching the brain’s sensory cortex. Only the cause is absent.
3D Observation: The most visually striking sequence in this simulation is the comparison between normal signal propagation and paresthetic firing. Normal signals shown as smooth, regular waves traveling from receptor to cortex — organized, purposeful, proportional. Paresthetic signals shown as irregular, spontaneous bursts — some propagating, some failing, some traveling backward — producing the characteristic uneven, variable intensity of the pins and needles sensation. The nervous system’s signal-to-noise ratio shown collapsing — the “noise” becoming the signal.

Stage 1: The Neurological Mechanisms — What Causes Paresthesia
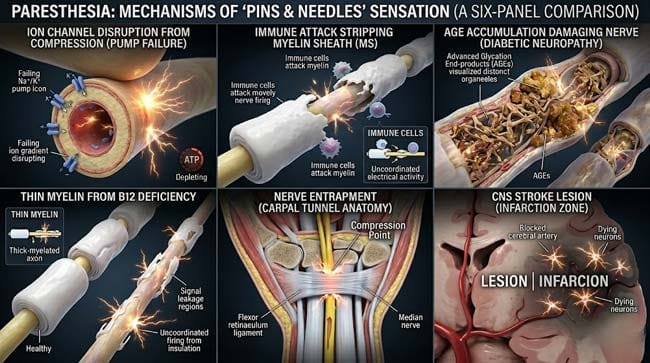
Paresthesia can be produced by disruption at any point along the sensory pathway — from the peripheral receptor to the sensory cortex. In our 3D neurological model, I identified six distinct mechanisms that produce paresthetic symptoms:
Mechanism 1 — Ion Channel Disruption (Positional/Transient)
The most common cause of acute paresthesia. Compression-induced ischemia shown causing sodium-potassium pump failure — membrane potential destabilization producing spontaneous firing during both the compressed (if partial) and recovery phases. This is the mechanism behind leg falling asleep — covered in detail in our previous article.
Mechanism 2 — Demyelination
In conditions like multiple sclerosis, the myelin sheath shown being attacked by the immune system — shown as the insulating white coating progressively thinning and developing gaps. Without complete myelination, saltatory conduction fails — signals shown slowing, failing, or becoming distorted.
In our 3D demyelination model, two key phenomena shown:
Ectopic impulse generation: Demyelinated axon segments shown becoming hypersensitive — the exposed axon membrane shown generating spontaneous action potentials that were previously suppressed by the myelin insulation.
Ephaptic transmission: Closely adjacent demyelinated fibers shown creating electrical cross-talk — signals shown jumping between fibers and producing paresthetic sensations in areas not corresponding to the original nerve’s territory.
Mechanism 3 — Metabolic Nerve Damage (Diabetic Neuropathy)
Chronic hyperglycemia shown having multiple damaging effects on peripheral nerves:
- Advanced glycation end products (AGEs) shown accumulating in nerve sheaths — cross-linking proteins and stiffening the nerve’s structural components
- Sorbitol accumulation shown in Schwann cells (myelin-producing cells) — osmotically damaging these cells and reducing their ability to maintain myelin
- Reduced nitric oxide shown impairing vasa nervorum vasodilation — creating chronic mild ischemia similar to positional compression but continuous
The result shown as diffuse small fiber neuropathy — predominantly affecting C fibers and A-delta fibers, producing the characteristic burning paresthesia of diabetic neuropathy that typically starts in the feet.
Mechanism 4 — Vitamin Deficiency (B12 Neuropathy)
Vitamin B12 is essential for myelin synthesis. Without adequate B12, shown as Schwann cells unable to produce or maintain myelin — the myelin sheath shown progressively thinning across all myelinated fibers. The resulting paresthesia shown as bilateral symmetric tingling, typically starting in the hands and feet — the classic glove and stocking distribution of B12 deficiency neuropathy.
Mechanism 5 — Nerve Entrapment
Physical compression of a nerve at a specific anatomical narrowing — such as the carpal tunnel (median nerve), cubital tunnel (ulnar nerve), or tarsal tunnel (tibial nerve). Unlike positional compression that is temporary, entrapment shown causing ongoing intermittent compression with repeated cycles of ischemia and recovery — shown as recurrent paresthesia in the nerve’s specific distribution.
Mechanism 6 — Central Nervous System Lesions
Lesions in the spinal cord or brain (from stroke, MS plaques, tumors, or spinal compression) shown disrupting sensory pathway function centrally — producing paresthesia in the body regions represented by the affected neural tissue. Central paresthesia often shown with a sharp anatomical boundary — a clear dermatomal or hemibody distribution that can precisely localize the lesion.
| Paresthesia Mechanism | Cause | 3D Visualization | Clinical Example |
|---|---|---|---|
| Ion channel disruption | Ischemia from compression | Pump failure, spontaneous firing | Leg falling asleep |
| Demyelination | Immune attack on myelin | Ectopic impulse generation, cross-talk | Multiple sclerosis |
| Metabolic damage | Chronic hyperglycemia | AGE accumulation, small fiber loss | Diabetic neuropathy |
| Vitamin deficiency | B12 absence — myelin failure | Progressive myelin thinning | B12 neuropathy |
| Nerve entrapment | Anatomical compression | Repeated ischemia cycles | Carpal tunnel syndrome |
| CNS lesion | Infarction, demyelination, tumor | Central pathway interruption | Stroke, MS plaque |
Common Medical Causes of Chronic Paresthesia:
| Condition | Mechanism | Distribution | Key Feature |
|---|---|---|---|
| Diabetic neuropathy | Metabolic nerve damage | Glove and stocking | Burning, worse at night |
| B12 deficiency | Myelin synthesis failure | Glove and stocking | Subacute onset |
| Multiple sclerosis | Demyelination | Variable — follows MS plaques | Relapsing-remitting |
| Carpal tunnel syndrome | Median nerve entrapment | Hand — thumb, index, middle | Worse at night |
| Cervical myelopathy | Spinal cord compression | Below compression level | Gait difficulty |
| Stroke | CNS infarction | Hemibody | Sudden onset |
| Hypothyroidism | Metabolic neuropathy | Diffuse, hands and feet | Associated fatigue |
| Alcohol neuropathy | Toxic nerve damage | Glove and stocking | Associated with alcohol use |
According to the National Institute of Neurological Disorders and Stroke (NINDS), paresthesia is one of the most common neurological complaints in clinical medicine — with chronic paresthesia being the presenting symptom of numerous conditions ranging from readily treatable deficiencies to serious neurological diseases requiring urgent intervention. NINDS: Paresthesia Information
Stage 2: When Paresthesia Is Serious — Red Flags and Emergency Signs
The Onset Pattern — The Most Important Diagnostic Clue:
| Onset Pattern | Most Likely Cause | Urgency | 3D Mechanism |
|---|---|---|---|
| Sudden (seconds) | Stroke, TIA, spinal injury | 🔴 EMERGENCY | Central pathway interruption |
| Acute (minutes–hours) | Nerve compression, migraine aura | 🟡 Urgent if new | Ion gradient disruption |
| Subacute (days–weeks) | B12/folate deficiency, medication | 🟡 Medical evaluation | Progressive myelin damage |
| Chronic progressive | Diabetes, alcohol, peripheral neuropathy | 🟡 Medical evaluation | Ongoing metabolic damage |
| Relapsing-remitting | Multiple sclerosis | 🟡 Neurological referral | Demyelination episodes |
The Emergency Red Flags:
These symptoms require immediate emergency evaluation:
- 🚨 Sudden onset paresthesia on one side of the body (face, arm, leg) — stroke until proven otherwise
- 🚨 Paresthesia following head or neck trauma
- 🚨 Ascending paresthesia (rising from feet upward) — Guillain-Barré syndrome
- 🚨 Paresthesia with muscle weakness — nerve or spinal cord involvement
- 🚨 Paresthesia with bowel or bladder dysfunction — spinal cord compression
- 🚨 Paresthesia with vision changes — multiple sclerosis or stroke
- 🚨 Sudden paresthesia with facial drooping or speech difficulty — stroke
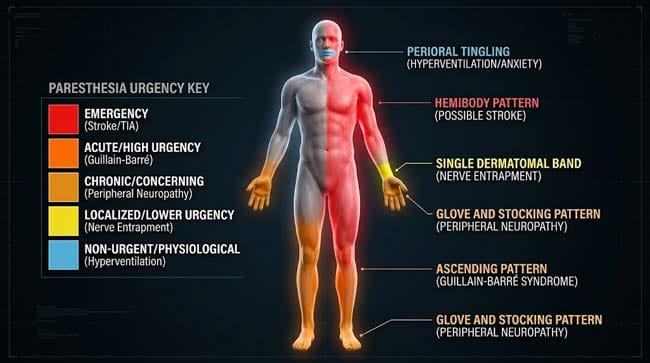
The Distribution Guide — Where It Tingling Tells You Where the Problem Is:
In our 3D anatomical mapping model, I showed how paresthesia distribution localizes the neurological problem:
Glove and stocking distribution (hands and feet symmetrically) → peripheral neuropathy → look for diabetes, B12 deficiency, alcohol
Single limb in a nerve distribution → nerve entrapment or radiculopathy → look for carpal tunnel, disc herniation
Dermatomal distribution (following a specific spinal nerve root) → radiculopathy → look for disc herniation, spinal stenosis
Hemibody (one entire side of body) → central nervous system lesion → look for stroke, MS plaque
Below a specific level on both sides → spinal cord lesion → look for myelopathy, spinal cord compression
Perioral and bilateral hands → hyperventilation → respiratory alkalosis causing ionized calcium reduction
Stage 3: Diagnosis and Treatment — Finding and Fixing the Source
The Diagnostic Approach:
The diagnostic approach to paresthesia follows the neurological principle of localization — determining where in the nervous system the problem originates before determining what is causing it.
Step 1 — Clinical History The most important diagnostic tool — onset, distribution, character (burning vs. tingling vs. numbness), associated symptoms, and medical history. In the 3D clinical model, I showed how a careful history narrows the diagnostic differential from 30+ possible conditions to 2–3 most likely causes before any testing.
Step 2 — Physical Examination Neurological examination shown assessing:
- Sensation: Light touch, pinprick, temperature, vibration, proprioception
- Reflexes: Reduced reflexes shown indicating peripheral neuropathy; hyperreflexia shown indicating upper motor neuron lesion
- Motor function: Weakness pattern shown localizing the lesion level
- Coordination: Cerebellar and proprioceptive testing
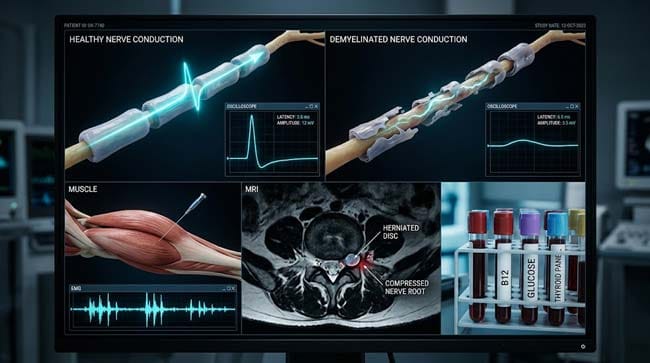
Step 3 — Investigations
| Investigation | What It Shows | Best For |
|---|---|---|
| Blood glucose / HbA1c | Diabetes | Diabetic neuropathy |
| Vitamin B12 level | B12 deficiency | B12 neuropathy |
| Thyroid function tests | Hypothyroidism | Thyroid neuropathy |
| Nerve conduction studies (NCS) | Nerve damage type and location | All neuropathies |
| Electromyography (EMG) | Muscle denervation | Motor involvement |
| MRI brain/spine | CNS lesions, disc herniation | MS, stroke, myelopathy |
| CSF analysis | Inflammatory/infectious causes | Guillain-Barré, MS |
Treatment by Cause:
| Cause | Treatment | Expected Outcome |
|---|---|---|
| Positional compression | Change position | Complete resolution in minutes |
| B12 deficiency | B12 supplementation | Significant improvement in weeks |
| Diabetic neuropathy | Blood glucose optimization + gabapentin/pregabalin | Stabilization, partial improvement |
| Carpal tunnel syndrome | Wrist splints → steroid injection → surgery | Resolution with appropriate treatment |
| MS-related | Disease-modifying therapy + symptomatic treatment | Reduced relapse frequency |
| Stroke | Acute thrombolysis → rehabilitation | Variable — depends on lesion size |
| Guillain-Barré | IVIG or plasmapheresis | Recovery over weeks to months |
According to the Mayo Clinic, the prognosis of paresthesia depends entirely on identifying and treating the underlying cause — with conditions like B12 deficiency responding dramatically to supplementation while others like established diabetic neuropathy requiring ongoing management rather than cure. Mayo Clinic: Numbness and Tingling — When to See a Doctor
FAQ: What Is Paresthesia?
Q1: Is paresthesia always a symptom of something serious? No — the vast majority of paresthesia experienced by healthy people is transient, positional, and completely benign. Leg falling asleep, arm going numb from sleeping in a certain position, and hand tingling from prolonged typing are all forms of paresthesia that require no medical attention. The pattern that warrants evaluation is paresthesia that is persistent (not resolving within minutes), recurrent without obvious positional cause, progressive over time, or associated with weakness, balance problems, or other neurological symptoms.
Q2: Can anxiety cause paresthesia? Yes — anxiety-related hyperventilation produces paresthesia through a specific physiological mechanism. Rapid breathing shown causing CO2 levels in the blood to drop — producing respiratory alkalosis. Alkalosis shown altering calcium ion binding to albumin — reducing ionized calcium levels. Low ionized calcium shown increasing peripheral nerve excitability — producing spontaneous firing and the characteristic tingling of hyperventilation, typically around the mouth and in the hands. Controlled breathing that restores normal CO2 levels rapidly resolves this paresthesia.
Q3: Why does paresthesia from nerve compression always start as numbness and end with pins and needles — not the reverse? The sequence reflects the differential vulnerability of nerve fiber types. C fibers (smallest, unmyelinated) fail first under compression — producing initial numbness as pain and temperature sensation are lost first. A-beta fibers (touch and pressure) fail progressively. During recovery, the same fibers recover in reverse order — A-beta fibers recover before C fibers. The pins and needles occur because A-beta fibers are firing spontaneously during their recovery while C fibers are still recovering — the brain perceives A-beta spontaneous signals as the prickling sensation of pins and needles.
Q4: Can paresthesia be treated? Treatment depends entirely on the cause. Transient positional paresthesia requires only position change. B12 deficiency paresthesia resolves with B12 supplementation — often dramatically within weeks. Diabetic neuropathy paresthesia is managed by optimizing blood sugar control and may be treated symptomatically with medications like gabapentin or pregabalin that reduce nerve excitability. MS-related paresthesia is managed as part of the overall MS treatment plan. Nerve entrapment paresthesia may require surgical decompression for definitive treatment.
Q5: Why do some people feel pins and needles when they are nervous or scared? Adrenaline release during fear activates the sympathetic nervous system — producing peripheral vasoconstriction that temporarily reduces blood flow to the skin and peripheral nerves. This mild, brief ischemia shown producing transient paresthesia — particularly in the extremities. Additionally, the hyperventilation that often accompanies anxiety produces the respiratory alkalosis mechanism described above. The combination of sympathetic vasoconstriction and hyperventilation can produce quite prominent paresthesia during acute anxiety or panic.
Conclusion: When the Nervous System Speaks Without Being Asked
Paresthesia is the nervous system producing sensation without external cause — signal without stimulus. In its benign form, it is the familiar companion of anyone who has ever sat too long in one position. In its chronic form, it is a clinically vital symptom — a distress signal from nerve tissue that is being damaged, compressed, or metabolically compromised.
In 3D, visualizing the spectrum of paresthesia mechanisms — from the simple ion gradient disruption of positional compression to the immune-mediated myelin destruction of multiple sclerosis to the metabolic devastation of diabetic neuropathy — reveals why the same symptom can mean anything from “shift position” to “call an ambulance.”
The symptom is the same. The cause, the urgency, and the treatment are completely different. Understanding which category your paresthesia falls into is the most important neurological self-assessment skill most people never develop.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured spontaneous nerve firing dynamics and demyelination progression |
| Material/Shader | Subsurface Scattering (SSS) | Simulating nerve fiber, myelin sheath, and CNS tissue visualization |
| Physics Engine | Volumetric Particle System + Electrostatic | Visualized action potential propagation failure, ion channel disruption |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of paresthesia mechanisms and clinical significance |
Read more on Why Does Your Leg Fall Asleep?
Pingback: Why Does Your Leg Fall Asleep? The 3D Nerve Science