The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore fecaloma — visualizing the formation of compacted fecal stones, their mechanical effects on surrounding organs, diagnostic imaging findings, and the medical and surgical removal procedures used to treat this extreme consequence of chronic constipation. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Is a Fecaloma? (The Atomic Answer)
A fecaloma is the extreme endpoint of chronic stool retention — a rock-hard, compacted mass of desiccated feces that has accumulated and hardened to the point where normal passage is impossible and medical intervention is required.
- The Formation: Fecaloma forms when stool remains in the colon or rectum for extended periods — days to weeks — while the large intestine continuously extracts water from it. The progressive desiccation transforms soft feces into increasingly dense, stone-like masses that can grow to the size of a grapefruit or larger.
- The Composition: A fully formed fecaloma is not simply dry stool — it is a partially mineralized composite of desiccated fecal organic matter, calcium phosphate and calcium carbonate deposits, compacted dead bacteria, mucus, and in some cases, swallowed foreign material incorporated over months.
- The Mechanical Effect: Large fecalomas exert significant pressure on adjacent structures — the bladder (causing urinary retention), the ureters (causing hydronephrosis), small bowel loops (causing obstruction), and the pelvic floor.
- The Treatment: Fecaloma treatment ranges from manual disimpaction under sedation to surgical colotomy in the most severe cases — with the choice determined by the size, location, and consistency of the mass.

My 3D Discovery: Rendering the “Stone Inside You”
When I was building the fecaloma cross-section model for this simulation, the most visually striking element was the geological layering visible in the simulation’s cross-section. Like a geological core sample or a pearl, a fecaloma shows distinct concentric layers — each representing a period of fecal accumulation.
In the 3D viewport, I rendered these layers at high resolution:
- Outer layers: Darker, more recently added material — still partially organic in composition
- Middle layers: More compressed, lighter in tone — older material with higher mineral content
- Inner core: Almost completely mineralized — calcium phosphate crystals shown as bright white geometric structures within the organic matrix
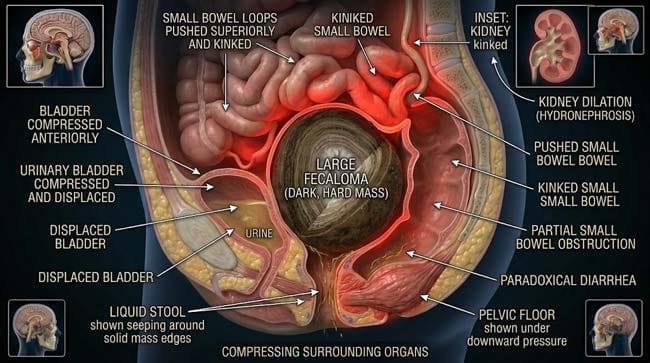
3D Observation: The most medically significant visualization in this simulation is the organ compression sequence. I rendered a large fecaloma in the rectosigmoid region and then showed its mechanical effects on surrounding structures in real time. The bladder shown being displaced anteriorly and compressed — urine flow shown being partially obstructed. The small bowel loops shown being pushed superiorly and kinked — intestinal transit shown being partially obstructed. The pelvic floor muscles shown under continuous downward pressure. The clinical consequences of a mass this size — urinary retention, nausea, abdominal pain, paradoxical diarrhea — become immediately understandable when the mechanical reality is visualized.
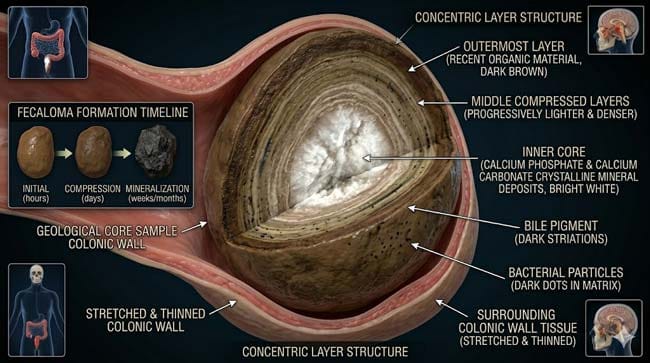
Stage 1: Fecaloma Formation — The Geological Process
Who Develops Fecalomas:
Fecaloma does not develop in healthy individuals with normal bowel function under typical circumstances. It occurs in specific high-risk populations:
Neurological conditions: Patients with spinal cord injury, multiple sclerosis, Parkinson’s disease, or severe stroke shown having impaired colonic motility and reduced defecation reflex — stool shown accumulating without adequate propulsive force to expel it.
Elderly and immobile patients: Reduced physical activity shown decreasing colonic motility. Dehydration shown accelerating water extraction from stool. Medication side effects (particularly opioid analgesics) shown dramatically reducing peristalsis.
Psychiatric conditions: Patients with severe depression, schizophrenia, or eating disorders shown sometimes ignoring defecation urges for extended periods or having severely disrupted gut-brain signaling.
Hirschsprung’s disease: Shown as congenital absence of ganglion cells in a segment of colon — the affected segment shown lacking peristaltic coordination, allowing stool to accumulate proximal to the aganglionic segment.
Chronic severe constipation: Long-term untreated constipation shown progressively developing the colonic inertia and rectal hyposensitivity that allows larger and larger fecal masses to accumulate without triggering adequate defecation reflexes.
The Formation Sequence:
In our 3D geological time-lapse, I rendered fecaloma development over a 6-week period:
Week 1 — Initial Accumulation: Normal stool shown arriving in the rectum but not being expelled. The rectal walls shown accommodating progressively larger volumes. The initial mass shown as soft — still easily passable if the defecation reflex were responded to.
Week 2 — Progressive Desiccation: Continuous aquaporin water extraction shown progressively hardening the accumulated mass. The outer surface shown drying and becoming resistant to normal peristaltic deformation. New stool shown arriving and being incorporated into the growing mass.
Week 3–4 — Mineralization Beginning: Calcium ions from intestinal secretions and bacterial metabolic products shown beginning to deposit within the organic matrix. In the 3D molecular model, calcium phosphate crystals shown nucleating at points of high organic concentration — the beginning of the mineralization process that distinguishes fecaloma from simple impacted stool.
Week 5–6 — Established Fecaloma: The mass shown reaching a size and consistency where normal passage is mechanically impossible — too large for the anal canal, too hard to be moved by peristalsis. The composition shown as a true composite material — organic desiccated feces with a mineral matrix, encased in layers of progressively harder material.
The Composition Analysis:
| Fecaloma Component | Origin | % by Mass (Approximate) | 3D Visualization |
|---|---|---|---|
| Desiccated organic matter | Fecal organic content | 40–50% | Brown fibrous matrix |
| Calcium phosphate | Intestinal secretions | 20–30% | White crystalline deposits |
| Calcium carbonate | Bacterial metabolism | 10–15% | Layered mineral structures |
| Dead bacteria | Colonic microbiome | 10–15% | Dark particles in matrix |
| Mucus | Colonic mucosa | 5–10% | Translucent binding layer |
| Bile pigments | Liver via bile | Variable | Dark coloration of layers |
According to the World Journal of Gastroenterology, fecalomas can reach sizes ranging from a few centimeters to over 15cm in diameter in extreme cases — with the largest documented cases requiring open surgical removal and weighing several kilograms. WJG: Fecaloma — Clinical Characteristics and Management
Stage 2: The Mechanical Consequences — What a Fecaloma Does to Surrounding Organs
The Pelvic Anatomy Context:
The pelvis is a confined bony space containing multiple critical structures in close proximity — the rectum, sigmoid colon, bladder, ureters, uterus (in females), prostate (in males), small bowel loops, and major pelvic blood vessels and nerves.
A large fecaloma occupying the rectosigmoid region shown exerting pressure on all of these structures simultaneously — the rigid mass shown unable to compress itself, instead shown displacing and compressing the softer surrounding structures.
Effect 1 — Bladder Compression and Urinary Retention:
In our 3D pelvic model, the bladder shown immediately anterior to the rectum. A large fecaloma shown pressing the posterior bladder wall forward — reducing bladder capacity and compressing the urethra.
Clinical consequence: acute urinary retention — shown as urine accumulating in the compressed bladder without being able to exit normally. Patients shown developing lower abdominal pain, inability to urinate, and bladder distension — symptoms that may initially confuse the clinical picture by appearing to be a urological rather than gastrointestinal problem.
Effect 2 — Ureteral Compression and Hydronephrosis:
In the most severe cases, the fecaloma shown compressing one or both ureters — the tubes connecting the kidneys to the bladder. Ureteral obstruction shown causing urine to back up into the kidney — producing hydronephrosis (kidney swelling from blocked outflow).
In the 3D renal model, the affected kidney shown progressively dilating as urine accumulates against the blockage — the renal pelvis and calyces shown expanding under back-pressure. Prolonged ureteral obstruction shown associated with permanent renal damage if not relieved.
Effect 3 — Small Bowel Obstruction:
Large fecalomas in the sigmoid colon shown compressing or kinking adjacent small bowel loops — producing partial or complete mechanical small bowel obstruction. Shown as small bowel loops shown dilating proximal to the compression point as intestinal gas and fluid accumulate.
Effect 4 — Paradoxical Diarrhea:
One of the most clinically confusing presentations of fecaloma is overflow incontinence — sometimes called paradoxical diarrhea. In our 3D model:
Liquid stool from the proximal colon shown unable to pass around the solid fecaloma — instead shown seeping around the edges of the solid mass and leaking out as watery, uncontrollable diarrhea. The patient shown experiencing what appears to be diarrhea — leading them (and sometimes clinicians) to believe they cannot have constipation or impaction.
This paradoxical presentation shown as the liquid component bypassing the solid mass — the clinical appearance of diarrhea coexisting with a massive fecal impaction.
| Organ Affected | Compression Mechanism | Clinical Consequence | 3D Visualization |
|---|---|---|---|
| Bladder | Direct posterior wall compression | Urinary retention, frequency | Bladder shown compressed anteriorly |
| Ureters | Lateral compression in severe cases | Hydronephrosis | Kidney shown dilating from back-pressure |
| Small bowel | Loop kinking and compression | Partial bowel obstruction | Bowel loops shown dilating proximal to compression |
| Pelvic floor | Continuous downward pressure | Pelvic floor weakness, prolapse risk | Floor shown under sustained downward load |
| Anal canal | Mass too large to pass | Outlet obstruction | Canal shown blocked by mass diameter |
Stage 3: Diagnosis and Treatment — Getting the Stone Out
Diagnosis:
Fecaloma diagnosis begins with clinical suspicion — a patient presenting with constipation, abdominal pain, urinary symptoms, or paradoxical diarrhea should be evaluated for fecal impaction.
Physical Examination: Digital rectal examination shown in the 3D model — the examining finger shown contacting a hard, immovable mass in the rectum. Palpable abdominal mass shown in the left lower quadrant for sigmoid fecalomas.
Imaging:
- Plain abdominal X-ray: Shown as the most common initial imaging — fecaloma shown as a rounded radiopaque mass in the expected colonic location
- CT scan: Shown as the definitive imaging — providing precise size, location, composition, and assessment of organ compression. The fecaloma shown as a high-density mass with characteristic heterogeneous composition on CT
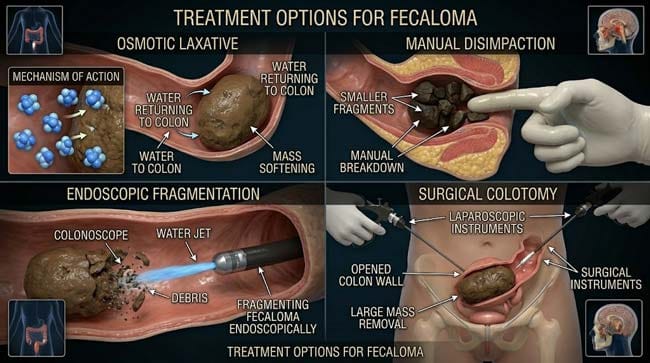
Treatment by Severity:
Level 1 — Oral and Rectal Laxative Therapy (Mild Cases)
For soft or early-stage impaction, shown as treatment with:
- Polyethylene glycol (PEG) — osmotic laxative shown drawing water back into the colon, softening the mass over 24–48 hours
- Phosphate enemas — shown delivering osmotically active solution directly to the rectum
- Docusate sodium — stool softener shown penetrating and softening the fecal mass
Level 2 — Manual Disimpaction (Moderate Cases)
For firmer impaction that does not respond to laxatives:
- Performed under sedation or spinal anesthesia in a clinical setting
- Clinician shown manually breaking up and removing the fecal mass digitally
- In the 3D procedure model, shown as a systematic fragmentation — breaking the solid mass into smaller pieces that can be removed manually or flushed with irrigation
Level 3 — Endoscopic Fragmentation (Moderate-Severe Cases)
For fecalomas in the sigmoid or more proximal colon:
- Colonoscope shown being advanced to the fecaloma location
- Specialized tools shown being used to fragment the mass — water jet fragmentation shown as the most effective technique
- Fragmented pieces shown being retrieved or allowed to pass naturally after fragmentation
Level 4 — Surgical Colotomy (Severe Cases)
For the largest fecalomas that cannot be reached endoscopically or removed manually:
- Shown as requiring laparoscopic or open abdominal surgery
- The colon shown being opened surgically — the fecaloma shown being removed through the colotomy incision
- The colon shown being repaired after removal — bowel continuity restored
| Treatment Level | Fecaloma Characteristics | Success Rate | 3D Procedure Visualization |
|---|---|---|---|
| Oral/rectal laxatives | Soft to moderately firm, accessible | 70–80% for appropriate cases | Osmotic water return to colon |
| Manual disimpaction | Firm but reachable rectally | 85–90% | Digital fragmentation and removal |
| Endoscopic fragmentation | Hard, sigmoid or proximal location | 80–85% | Colonoscope with water jet |
| Surgical colotomy | Very large or inaccessible | 95%+ | Open or laparoscopic colon surgery |
According to the American Society of Colon and Rectal Surgeons, prevention of fecaloma through adequate hydration, dietary fiber, regular physical activity, and prompt treatment of constipation is significantly preferable to treatment — with surgical intervention for established large fecalomas carrying perioperative risks including infection, anastomotic leak, and prolonged recovery. ASCRS: Constipation and Fecal Impaction Guidelines
FAQ: Fecaloma — What Is It?
Q1: How do I know if I have a fecaloma versus regular constipation? Regular constipation involves difficulty passing stool but the stool can eventually be passed. Fecaloma presents with complete inability to pass stool despite urging and straining, palpable abdominal mass, and often paradoxical watery leakage around the obstruction. Associated symptoms — urinary retention, abdominal distension, and nausea — suggest a mass large enough to compress adjacent organs. Any constipation lasting more than 7–10 days without any stool passage, particularly in elderly or neurologically impaired individuals, warrants medical evaluation for impaction.
Q2: Can a fecaloma be life-threatening? Yes — in extreme cases. The most serious complications include: stercoral perforation (the fecaloma eroding through the colonic wall), complete bowel obstruction, ureteral obstruction causing acute kidney failure, and sepsis from bacterial translocation across the compromised colonic mucosa under pressure. Stercoral perforation — shown in the simulation as the fecaloma’s pressure causing ischemic necrosis and full-thickness hole in the colonic wall — carries mortality rates of 35–57% even with emergency surgical intervention.
Q3: Can diet prevent fecaloma? Yes — dietary prevention is straightforward and highly effective. Adequate daily fiber intake (25–38g for adults) maintains stool bulk and softness. Adequate hydration (1.5–2 liters of water daily) prevents the excessive desiccation that drives fecaloma formation. Regular physical activity maintains colonic motility. For high-risk individuals (elderly, neurological conditions, chronic opioid use), regular use of osmotic laxatives like polyethylene glycol as a preventive measure is recommended by gastroenterologists.
Q4: Can children develop fecalomas? Yes — pediatric fecaloma is an important clinical entity, occurring most commonly in children with Hirschsprung’s disease, anorectal malformations, or severe functional constipation with stool withholding behavior. In children, the diagnosis requires particular awareness because the presenting symptoms — abdominal distension, poor appetite, soiling — may initially be attributed to other causes. Pediatric fecaloma treatment follows similar principles but requires age-appropriate dosing and technique modification.
Q5: After a fecaloma is removed, does the bowel return to normal? In most cases, yes — with appropriate post-treatment management. The colon’s mucosal function typically recovers once the chronic obstruction is relieved. However, rectal hyposensitivity (reduced ability to sense rectal fullness) may persist for weeks to months, requiring bowel retraining with scheduled toilet times and osmotic laxatives to prevent recurrence. The underlying cause — whether neurological, medication-related, or behavioral — must be addressed to prevent fecaloma recurrence, which is common without addressing root causes.
Conclusion: When Biology’s Patience Runs Out
Fecaloma represents the endpoint of a process that the body resists for as long as it can — accommodating, expanding, reabsorbing water, attempting peristalsis against an increasingly immovable mass. Eventually, the physics of a stone inside a biological tube overcomes the body’s adaptive capacity.
In 3D, rendering the geological cross-section of a fully formed fecaloma — the concentric layers, the mineral deposits, the partially calcified organic matrix — and then showing its mechanical effect on the bladder, ureters, and small bowel in the confined pelvic space makes the clinical consequences immediately understandable.
The human body’s most powerful self-cleaning system — the digestive tract — can be overwhelmed by its own substrate when motility fails and retention persists. The result is not simply a large stool. It is a geological formation inside a biological cavity.
Prevention requires only water, fiber, movement, and attention to the body’s signals. The alternative requires surgery.
Further Study & External Research
- WJG — Fecaloma Clinical Characteristics and Management
- ASCRS — Constipation and Fecal Impaction Guidelines
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured fecaloma formation and organ compression mechanics |
| Material/Shader | Subsurface Scattering (SSS) + Crystalline Shader | Simulating fecaloma mineral composition and surrounding tissue compression |
| Physics Engine | Rigid Body + Fluid Dynamics | Visualized mass formation, organ displacement, and treatment fluid mechanics |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of fecaloma formation, consequences, and treatment |
Read more on What Happens If You Hold Your Poop?