The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore Q-tip ear damage — visualizing the complete spectrum of injuries cotton swabs cause to the ear canal, from cerumen impaction and microbiome disruption to tympanic membrane perforation and ossicular chain trauma. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Q-Tip Ear Damage Looks Like? (The Atomic Answer)
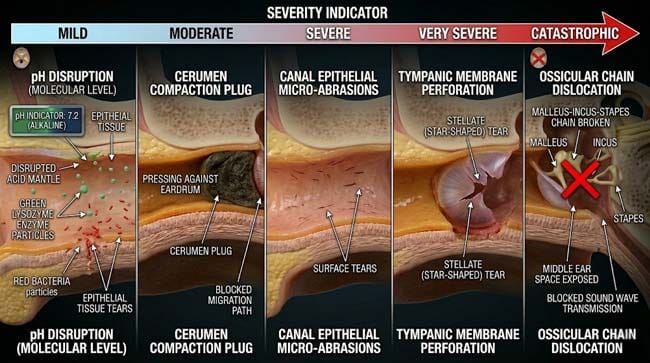
Q-tip ear damage is not a single injury — it is a spectrum of damage ranging from gradual microbiome disruption to acute tympanic membrane perforation. Most people who use Q-tips regularly are experiencing the milder forms of damage without realizing it.
- Level 1 — Microbiome Disruption: Every Q-tip insertion removes the acidic cerumen layer that maintains the ear canal’s antimicrobial environment — increasing susceptibility to otitis externa (swimmer’s ear) by disrupting the pH barrier and removing defensive proteins.
- Level 2 — Cerumen Impaction: Chronic Q-tip use compacts earwax into increasingly dense plugs that press against the tympanic membrane — causing progressive conductive hearing loss, tinnitus, and ear fullness that worsens with each insertion.
- Level 3 — Canal Trauma: The cotton tip’s abrasive action and the Q-tip’s rigid stem can cause microscopic lacerations in the thin, sensitive skin of the inner ear canal — creating entry points for infection.
- Level 4 — Tympanic Membrane Perforation: Direct contact with the eardrum — particularly during startling events — can perforate the membrane, causing immediate severe pain, significant hearing loss, and risk of middle ear infection.
- Level 5 — Ossicular Chain Damage: In the most severe cases, forceful Q-tip insertion can dislocate or fracture the ossicular chain (the three tiny bones that transmit sound) — causing permanent sensorineural hearing loss.

My 3D Discovery: Rendering the Five Levels of Damage
When I was building the comprehensive Q-tip damage model for this simulation, I decided to render all five damage levels simultaneously in a side-by-side timeline — showing how the same tool causes completely different types of injury depending on insertion depth, force, and frequency.
The most visually striking contrast was between Level 1 and Level 5. Level 1 damage — microbiome disruption — is invisible at normal scale, shown only at the molecular level as pH changes and antimicrobial protein removal. Level 5 damage — ossicular chain fracture — is catastrophic at the anatomical scale, shown as the entire middle ear sound transmission system failing after a single forceful insertion.
3D Observation: The most sobering sequence in this simulation is the ossicular chain damage visualization. The ossicular chain consists of three bones — the malleus (hammer), incus (anvil), and stapes (stirrup) — arranged in a precise mechanical linkage that amplifies sound 22-fold before it reaches the inner ear. In the animation, showing these three tiny bones — the smallest in the entire human body — being disrupted by a cotton swab puts the fragility of the hearing apparatus in immediate perspective. These bones cannot be repaired by the body. Once fractured or dislocated, surgical intervention is required — and outcomes are not guaranteed.
Stage 1: The Spectrum of Q-Tip Ear Damage — Five Levels
Level 1 — Microbiome and pH Disruption
The ear canal microbiome is a carefully balanced ecosystem — dominated by acidophilic bacteria like Corynebacterium and Staphylococcus epidermidis that thrive in cerumen’s pH 4.5–6.5 environment and actively compete against pathogenic species.
In our 3D microbiome model, I showed what happens with each Q-tip insertion:
Cerumen removal → pH neutralization The acidic cerumen shown being stripped from the canal wall. Without its protective coating, the canal pH shown rising toward neutral (7.0). In the animation, the previously hostile acid environment shown becoming increasingly hospitable to pathogenic bacteria and fungi.
Key pathogens that emerge in the absence of cerumen:
- Pseudomonas aeruginosa — shown as green rod-shaped bacteria — the primary cause of otitis externa, requiring an alkaline environment to colonize
- Candida albicans — shown as budding yeast cells — fungal colonizer that cannot establish in acidic cerumen-coated canals
- Staphylococcus aureus — shown as orange clusters — opportunistic pathogen that colonizes disrupted canal epithelium
In the time-lapse simulation, a clean, cerumen-stripped canal shown progressively colonized by pathogenic species over 48–72 hours — explaining the well-documented association between regular Q-tip use and recurrent otitis externa.
Level 2 — Cerumen Impaction (Progressive)
Already covered comprehensively in Stage 2 of the previous article — the compaction mechanism producing progressive hearing loss, tinnitus, and ear fullness.
Additional detail: In our 3D impaction model, I showed the vascular effect of severe impaction. A large cerumen plug pressing against the tympanic membrane shown exerting continuous pressure on the membrane’s blood supply — shown as capillaries in the outer tympanic membrane layer being compressed, reducing blood flow to the membrane. Chronic pressure from impacted cerumen can contribute to localized tympanic membrane thinning and increased perforation risk over time.
Level 3 — Canal Epithelial Trauma
The inner two-thirds of the ear canal is lined with extremely thin skin — lacking the protective hair follicles and thicker keratin layer of outer canal skin. This inner canal skin is highly sensitive and easily traumatized.
In our 3D canal epithelium model, I showed the microscopic effect of Q-tip abrasion:
Acute trauma: The cotton fibers shown creating microscopic surface abrasions — removing the superficial epithelial cell layer and exposing the underlying dermis. These micro-abrasions shown creating immediate pain signals through the dense auriculotemporal nerve supply.
Chronic trauma: Repeated Q-tip insertion shown producing a cycle of micro-trauma and attempted repair — with the repair process producing mild epithelial thickening and scarring over time. This chronic irritation shown contributing to the itch-scratch cycle that drives habitual Q-tip use.
The Itch-Scratch Paradox:
In the 3D cycle visualization, I showed why habitual Q-tip use becomes self-reinforcing:
- Q-tip removes cerumen → canal skin dries out → dryness causes itching
- Itching drives Q-tip insertion for relief → more cerumen removed → more drying
- Q-tip abrasion causes micro-inflammation → inflammation causes itching
- Cycle shown becoming progressively more entrenched with each insertion
| Damage Level | Mechanism | Timeline | Reversibility |
|---|---|---|---|
| Microbiome disruption | pH and antimicrobial protein removal | Immediate, per insertion | ✅ Reversible — cerumen regenerates |
| Cerumen impaction | Progressive compaction | Weeks to months | ✅ Reversible with professional removal |
| Canal epithelial trauma | Abrasion and drying | Per insertion, cumulative | ✅ Mostly reversible |
| Tympanic perforation | Direct membrane contact | Single event | ⚠️ Usually reversible, sometimes not |
| Ossicular chain damage | Forceful insertion | Single event | ❌ Rarely fully reversible |
Stage 2: Tympanic Membrane Perforation — The Acute Injury
Anatomy of the Tympanic Membrane:
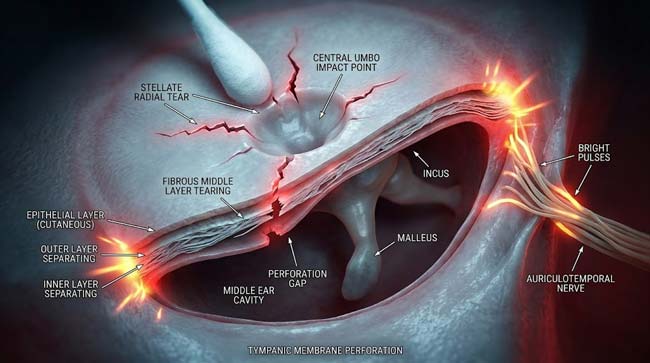
The tympanic membrane is a three-layer structure — approximately 9–10mm in diameter and 0.1mm thick at its center — one of the thinnest membranes in the human body.
In our 3D membrane model, I rendered its three layers:
- Lateral (outer) layer: Thin squamous epithelium — continuous with the ear canal skin
- Middle layer: Fibrous layer — radial and circular collagen fibers providing mechanical strength
- Medial (inner) layer: Mucosal layer — continuous with the middle ear mucosa
The membrane’s mechanical strength is concentrated in its fibrous middle layer. The central region (pars tensa) shown as the most taut and most vulnerable to perforation from direct contact.
The Perforation Mechanics:
In our 3D perforation simulation, I modeled three scenarios:
Scenario 1 — Gradual pressure (cerumen plug pushing against membrane): Progressive membrane deflection shown — the membrane bowing inward under constant impaction pressure. Over months, shown causing tympanosclerosis (membrane calcification) rather than acute perforation.
Scenario 2 — Direct Q-tip contact with moderate force: Cotton tip shown making contact with the central pars tensa. Stress concentration shown at the umbo (center point). At sufficient force, shown radial tearing from the umbo outward — producing a characteristic stellate (star-shaped) perforation pattern.
Scenario 3 — Startle response during Q-tip insertion (most common injury mechanism): This is the scenario responsible for the majority of Q-tip perforations. The Q-tip shown at mid-insertion — cotton tip not yet touching the membrane. A sudden movement (being bumped, hearing a loud noise, flinching from cold water) shown driving the Q-tip forward by 10–15mm in milliseconds. The perforation shown occurring before any protective reflex can activate.
Post-Perforation Consequences:
| Consequence | Mechanism | Timeline | 3D Visualization |
|---|---|---|---|
| Immediate severe pain | Tympanic membrane nerve supply | Instantaneous | Nerve pulse shown radiating from membrane |
| Conductive hearing loss | Reduced membrane vibration area | Immediate | Sound wave transmission shown reduced |
| Tinnitus | Altered acoustic mechanics | Immediate to days | Standing wave patterns shown disrupted |
| Middle ear exposure | Open pathway to middle ear | Until healed | Bacterial access shown to previously sealed space |
| Otitis media risk | Contamination of middle ear | Days to weeks | Bacteria shown entering exposed middle ear |
Stage 3: Ossicular Chain Damage — The Worst Case
The Ossicular Chain:
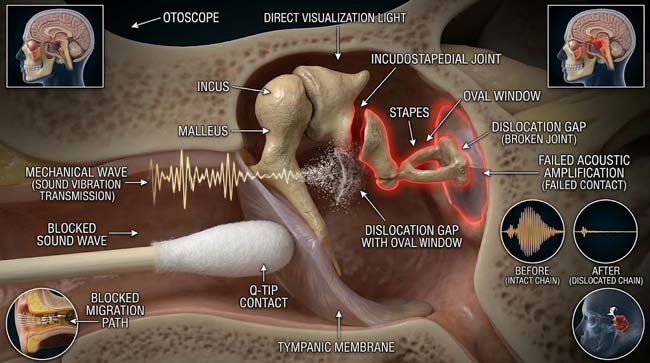
The ossicular chain consists of three bones — malleus, incus, and stapes — linked in series across the middle ear cavity. They transmit and amplify sound vibrations from the tympanic membrane to the oval window (entry to the inner ear).
In our 3D ossicular model, I rendered these bones at precise scale:
- Malleus: Approximately 8mm long — the handle shown embedded in the tympanic membrane
- Incus: Approximately 7mm long — linking malleus to stapes
- Stapes: Approximately 3mm long and 2mm wide — the smallest bone in the human body, shown fitting into the oval window
Why Ossicular Damage is Catastrophic:
In our acoustic amplification model, I showed the ossicular chain’s function:
The chain provides a mechanical advantage of approximately 22:1 — amplifying sound pressure 22 times between the tympanic membrane and the oval window. Without this amplification, the cochlea would receive insufficient signal for normal hearing — producing a 55–60 dB conductive hearing loss (the threshold between moderate and severe hearing loss).
The Ossicular Damage Mechanisms:
Incudostapedial Joint Dislocation: The most common ossicular injury from Q-tip insertion. In the 3D model, a forceful Q-tip pushing the tympanic membrane inward shown transmitting force through the malleus to the incus — if the force is sufficient, the incudostapedial joint shown subluxing (partially dislocating) or fully dislocating.
In the animation, this dislocation appears as the mechanical chain suddenly losing its rigid connection — vibrations shown no longer being efficiently transmitted through the gap.
Stapes Subluxation: In severe cases, force transmitted to the stapes shown displacing it into the oval window — potentially penetrating the inner ear membrane (perilymph fistula). This shown as the most severe outcome — combining conductive hearing loss with inner ear damage producing mixed conductive and sensorineural hearing loss.
The Permanence of Ossicular Damage:
Unlike tympanic membrane perforations (which often heal spontaneously), ossicular dislocations do not self-correct. In our 3D surgical model, I showed the required surgical intervention — ossiculoplasty — shown as a delicate procedure requiring general anesthesia, operating microscope visualization, and prosthetic ossicle placement.
Outcomes of ossiculoplasty are variable — full hearing restoration is not guaranteed, and the surgical risk includes total sensorineural hearing loss from inner ear trauma during the procedure.
According to the American Journal of Otolaryngology, iatrogenic (self-inflicted) ossicular chain damage from cotton swab use represents a significant but underreported cause of conductive hearing loss — with many patients presenting months to years after the initial injury, unaware that their hearing loss originated from ear cleaning habits. AJO: Cotton Swab Injuries to the Ear
FAQ: Q-Tip Ear Damage
Q1: How do I know if I have damaged my ears with Q-tips? Warning signs of Q-tip related ear damage include: progressive hearing muffling or loss, sensation of ear fullness that does not resolve, tinnitus (ringing, buzzing, or roaring sounds), recurrent ear infections (otitis externa), pain or discomfort after ear cleaning, and sudden hearing loss after a Q-tip insertion event. Any sudden significant hearing change after Q-tip use should be evaluated by an ENT specialist immediately — this could indicate tympanic membrane perforation or ossicular damage.
Q2: If my tympanic membrane is perforated by a Q-tip, what should I do? Seek medical evaluation promptly — ideally on the same day. Keep the ear dry — no swimming, no shower water in the ear, use cotton wool with petroleum jelly as a barrier during showering. Do not insert anything into the ear. Most small perforations (less than 25% of membrane area) heal spontaneously within 4–8 weeks with appropriate care. Larger perforations or those showing signs of infection require ENT evaluation for potential surgical repair.
Q3: Can the hearing loss from cerumen impaction caused by Q-tips be reversed? Yes — cerumen impaction is one of the most reversible causes of hearing loss. Professional cerumen removal — via microsuction, irrigation, or manual removal with a curette — restores hearing to pre-impaction levels in the vast majority of cases. The key is ensuring complete removal, which should be performed by a healthcare provider rather than attempted at home. After removal, maintaining cerumen naturally and avoiding Q-tip insertion prevents recurrence.
Q4: Are there any safe ear cleaning tools? Several alternatives to Q-tips exist for people who genuinely need cerumen management: cerumen softening drops (over-the-counter carbamide peroxide solutions), ear irrigation kits with specially designed bulb syringes that direct water safely along the canal wall, and professional microsuction or irrigation performed by a healthcare provider. None of these should involve anything being inserted past the entrance of the ear canal. The outer pinna can be cleaned with a standard cotton swab without entering the canal.
Q5: Why does the Q-tip packaging say “do not insert into ear canal” if everyone uses them for ears? This warning has appeared on Q-tip packaging since the 1970s — added after the US Consumer Product Safety Commission documented the extent of ear injuries caused by the product. Despite this explicit warning, surveys suggest that over 68% of Q-tip users use them specifically to clean ear canals — the behavior the warning explicitly prohibits. This represents one of the most widely ignored product warnings in consumer goods history.
Conclusion: The Tool That Causes the Problem It Tries to Solve
Q-tip ear damage exists on a spectrum — from the invisible microbiome disruption that happens with every insertion to the catastrophic ossicular chain injuries that occur in worst-case scenarios. Most users experience the milder forms continuously without awareness, while a significant minority experience acute injuries that require medical intervention.
In 3D, rendering all five damage levels simultaneously — from the molecular-scale pH disruption to the anatomical-scale ossicular chain dislocation — makes the complete picture of Q-tip ear damage visible in a single simulation. The tool designed to clean creates impaction. The cleaning motion creates the itch-scratch cycle that drives habitual use. And the canal designed to clean itself needs only to be left alone.
The ears were here before Q-tips existed. They will continue working without them.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured ossicular chain mechanics and tympanic membrane perforation dynamics |
| Material/Shader | Subsurface Scattering (SSS) | Simulating ear canal tissue, membrane translucency, and bone microstructure |
| Physics Engine | Finite Element + Rigid Body Dynamics | Visualized membrane stress distribution, ossicular joint mechanics, perforation propagation |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of complete Q-tip ear damage spectrum |
Read more on Why You Should Not Clean Ears With Q-Tips
Pingback: Why You Should Not Clean Ears With Q Tips: 3D Ear Science