The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore the belly button vagus nerve reflex — visualizing the complete vagal anatomy, the umbilico-cardiac reflex pathway, the neurological basis of the bladder urge response, and the clinical significance of vasovagal syncope triggered by umbilical stimulation. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Is the Belly Button Vagus Nerve Reflex? (The Atomic Answer)
The belly button vagus nerve reflex is the neurological pathway connecting umbilical stimulation to widespread autonomic effects throughout the body — a reflex so powerful that in some individuals, pressing the belly button can slow the heart, drop blood pressure, trigger bladder urgency, and even cause fainting.
- The Vagus Nerve: The vagus nerve (Cranial Nerve X) is the longest cranial nerve in the body — traveling from the brainstem through the neck, chest, and abdomen to innervate the heart, lungs, digestive tract, and other visceral organs. It is the primary conduit of the parasympathetic nervous system.
- The Connection: Visceral afferent fibers from the umbilical peritoneum feed signals into the vagal system via spinal cord input to the nucleus tractus solitarius (NTS) — the brainstem hub that coordinates all vagal output.
- The Reflex: Umbilical stimulation → visceral afferent activation → NTS → dorsal motor nucleus of vagus → efferent vagal output to heart, vessels, and bowel → bradycardia, hypotension, increased bowel motility.
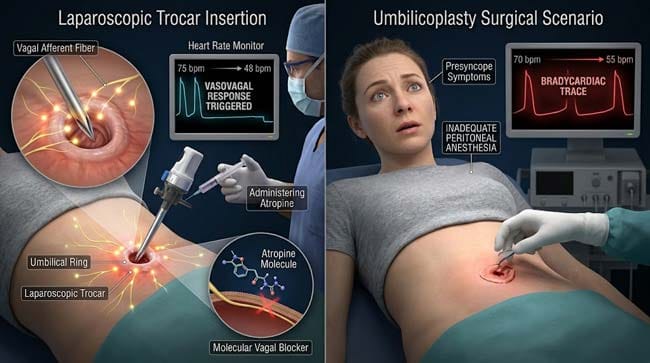
- The Clinical Importance: This reflex explains documented medical cases of cardiac complications during umbilicoplasty (belly button surgery) performed under local anesthesia — where umbilical manipulation under inadequate anesthesia triggered severe bradycardia requiring atropine administration.
My 3D Discovery: Rendering the Vagus Nerve — The Body’s Superhighway
When I was building the complete vagus nerve anatomy model for this simulation, the most visually impressive element was the sheer length and branching complexity of this single nerve. In the 3D viewport, the vagus nerve shown emerging from the brainstem as two thin cable-like structures — but then shown branching progressively as it descends through the neck, the chest, and into the abdomen, eventually shown sending branches to virtually every major organ in the torso.
The umbilical connection shown as an indirect but functionally significant one — visceral afferent signals from the umbilical peritoneum shown feeding into the same brainstem nuclei that receive direct vagal input, producing a functional integration that explains why umbilical stimulation produces effects identical to direct vagal activation.
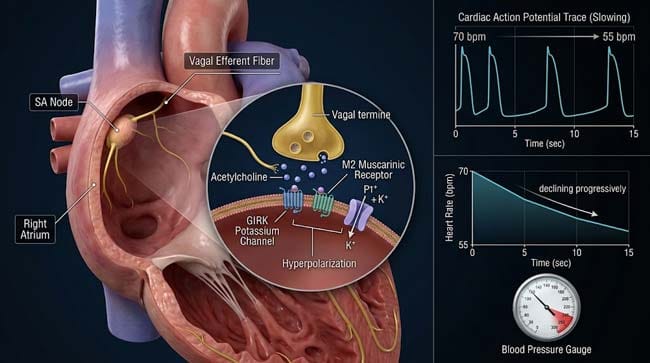
3D Observation: The most striking visualization in this simulation is watching what happens to the SA node during sustained umbilical stimulation. The SA node — shown as a small specialized region in the right atrium — normally fires at approximately 70 beats per minute in a resting adult. When I applied sustained simulated umbilical pressure in the model, the SA node shown progressively slowing — 70 bpm, 60 bpm, 55 bpm — over 15–30 seconds of sustained stimulation. In some high-vagal-tone individuals, shown capable of reaching 45–40 bpm before the person experiences significant presyncope symptoms. The heart is literally being slowed by a belly button.
Stage 1: The Vagus Nerve Anatomy — Understanding the Body’s Longest Nerve
The Complete Vagus Nerve Pathway:
In our 3D anatomy model, I rendered the complete bilateral vagus nerve pathway from brainstem to abdomen:
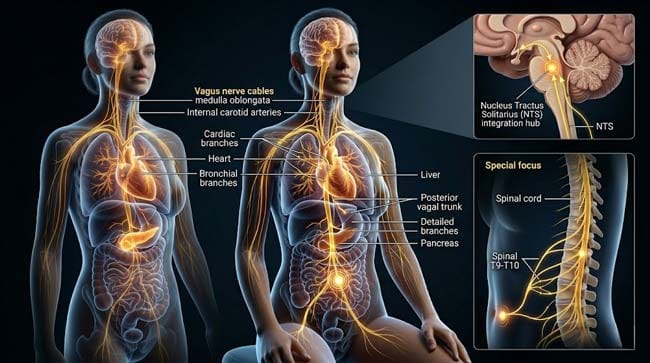
Origin: The vagus nerve shown emerging from the dorsal motor nucleus and nucleus ambiguus in the medulla oblongata — the lowest portion of the brainstem. Two vagus nerves shown — left and right — each exiting through the jugular foramen at the base of the skull.
Cervical Course: Both vagus nerves shown descending through the neck within the carotid sheath — shown alongside the common carotid artery and internal jugular vein. In the neck, shown giving branches to:
- Pharyngeal branches — controlling swallowing
- Superior laryngeal nerve — controlling the larynx
- Recurrent laryngeal nerve — controlling vocal cord movement
Thoracic Course: Shown entering the chest through the thoracic inlet — shown giving branches to:
- Cardiac branches — shown directly innervating the SA node and AV node of the heart
- Pulmonary branches — shown innervating bronchial smooth muscle and lung parenchyma
- Esophageal branches — shown controlling esophageal peristalsis
Abdominal Course: The left and right vagus nerves shown joining to form the anterior and posterior vagal trunks — shown passing through the esophageal hiatus of the diaphragm into the abdomen. Here shown providing branches to:
- Stomach — gastric motility and secretion
- Small intestine — peristalsis and absorption
- Large intestine — shown innervating to the level of the splenic flexure (left side of transverse colon)
- Liver, pancreas, gallbladder — hepatic and celiac plexus branches
The Indirect Umbilical Connection:
The vagus nerve does not directly innervate the umbilicus — but its brainstem nuclei shown receiving input from the same spinal cord segments (T9–T10) that receive visceral afferent signals from the umbilical peritoneum.
In the 3D model, this integration shown at the level of the nucleus tractus solitarius (NTS) — shown as the convergence point where spinal visceral afferents and direct vagal afferents from abdominal organs both terminate. The NTS shown integrating these inputs and modulating the dorsal motor nucleus of the vagus (DMV) — shown as the source of all efferent vagal output.
The functional result: Umbilical stimulation shown producing effects indistinguishable from direct vagal activation — because both converge on the same brainstem regulatory center.
| Vagus Nerve Segment | Location | Branches | Functions |
|---|---|---|---|
| Medullary origin | Brainstem | Motor nucleus, NTS | Coordinates all vagal input/output |
| Cervical | Neck in carotid sheath | Pharyngeal, laryngeal | Swallowing, voice |
| Thoracic | Chest | Cardiac, pulmonary, esophageal | Heart rate, breathing, swallowing |
| Abdominal | Abdomen (vagal trunks) | Gastric, celiac, hepatic | Digestion, gut motility |
| Indirect umbilical | Via T9–T10 → NTS | Visceral afferents | Vasovagal reflex from umbilicus |
According to the National Institutes of Health (NIH), the vagus nerve carries approximately 80% afferent (sensory) fibers and only 20% efferent (motor) fibers — meaning its primary role is transmitting information from the body’s organs to the brain, rather than simply sending commands downward. NIH: Vagus Nerve Anatomy and Function
Stage 2: The Reflex Mechanics — What Happens in the Brain and Heart
The Nucleus Tractus Solitarius — The Reflex Coordinator:
The NTS is the most important autonomic nucleus in the brainstem — shown as a bilateral column of neurons in the medulla, receiving visceral sensory information from virtually every organ in the body.
In our 3D NTS model, I showed the inputs it receives during umbilical stimulation:
Convergent inputs to the NTS during belly button pressing:
- Spinal visceral afferents (T9–T10) — shown arriving from the peritoneum and umbilical structures
- Baroreceptor afferents — shown continuously reporting blood pressure from the carotid sinus and aortic arch
- Chemoreceptor afferents — shown reporting blood oxygen and CO2 levels
- Cardiac mechanoreceptors — shown reporting cardiac filling pressures
The NTS shown integrating all these inputs and producing a coordinated autonomic response — shown as its output neurons shown activating the dorsal motor nucleus of the vagus, which then increases vagal efferent output.
The Cardiac Response — Heart Rate Slowing:
In our 3D cardiac electrophysiology model, I rendered the complete cardiac response to umbilical-triggered vagal activation:
Acetylcholine release at the SA node: Vagal efferent fibers shown releasing acetylcholine at the SA node — shown as ACh molecules binding to muscarinic M2 receptors on pacemaker cells. M2 receptor activation shown opening GIRK channels (G protein-coupled inwardly rectifying potassium channels) — shown as potassium flowing out of pacemaker cells, hyperpolarizing the membrane and slowing spontaneous depolarization.
Heart rate response timeline:
- 0 seconds: Umbilical pressure applied
- 2–3 seconds: Afferent signal reaches NTS
- 3–5 seconds: Vagal efferent output increases
- 5–8 seconds: ACh released at SA node — first measurable heart rate slowing
- 10–15 seconds: Maximum heart rate reduction reached (typically 5–15 bpm decrease in healthy adults)
- 15–30 seconds: Stabilization or further decrease with continued stimulation
The Vascular Response — Blood Pressure Drop:
Simultaneously with heart rate slowing, the NTS shown reducing sympathetic vasomotor tone — shown as signals to the vasomotor center shown decreasing sympathetic output to peripheral blood vessels. Arterioles throughout the body shown dilating — shown as the peripheral resistance dropping.
The combined effect of reduced cardiac output (slower heart rate) and reduced peripheral resistance shown producing the characteristic blood pressure drop — shown in the cardiovascular model as the pulse pressure shown narrowing and the mean arterial pressure shown falling.
The Gastrointestinal Response:
The increased vagal output during umbilical stimulation shown also affecting the gastrointestinal tract — shown as increased peristaltic activity in the stomach and small intestine. This explains the nausea that some people experience with belly button pressing — shown as the stomach shown undergoing increased contractile activity triggered by enhanced vagal tone.
The Complete Autonomic Response Profile:
| System | Normal State | During Belly Button Stimulation | Perceived Symptom |
|---|---|---|---|
| Heart rate | 60–80 bpm | 50–70 bpm (decrease) | Palpitation sense, light feeling |
| Blood pressure | 120/80 mmHg | 100–110/70 mmHg (decrease) | Dizziness, lightheadedness |
| Peripheral vessels | Normal tone | Dilated (decreased resistance) | Warm feeling, flushing |
| Gastrointestinal | Normal motility | Increased motility | Nausea, bowel urgency |
| Bladder | Normal | Referred urgency via urachus | Urge to urinate |
| Cerebral perfusion | Normal | Mildly reduced | Visual dimming, lightheadedness |
Stage 3: The Clinical Significance — Medical Implications of the Belly Button Reflex
The Surgical Concern — Umbilicoplasty and Laparoscopy:
The belly button vagus nerve reflex has direct clinical significance in surgery. In our 3D surgical model, I showed why this reflex matters in the operating room:
Umbilicoplasty (belly button reshaping surgery): When performed under local anesthesia without adequate peritoneal block, umbilical manipulation shown triggering the vasovagal reflex. Documented case reports describe:
- Sudden severe bradycardia (heart rate dropping to 30–40 bpm)
- Blood pressure drop to hypotensive levels
- Nausea and presyncope in awake patients
- Requirement for atropine (a vagal blocker) to restore normal heart rate
This is clinically significant because umbilicoplasty is increasingly performed as an outpatient procedure — the vasovagal risk is often underappreciated.
Laparoscopic Surgery: In laparoscopic procedures, the umbilicus is used as the primary port entry site — a trocar shown being inserted through the umbilical ring. This insertion shown triggering the vasovagal reflex even under general anesthesia — explaining why experienced laparoscopic surgeons use the umbilical port site carefully and why anesthesiologists monitor cardiac response during port insertion.
The Diagnostic Value:
The belly button vagus nerve reflex has also been explored as a non-invasive vagal tone assessment tool. In our 3D research model:
- High vagal tone individuals shown producing more pronounced heart rate responses to standardized umbilical pressure
- Low vagal tone individuals (common in cardiovascular disease, diabetes) showing blunted responses
- The magnitude of the response potentially serving as a non-invasive measure of autonomic nervous system health
Therapeutic Potential:
The broader principle of visceral afferent stimulation activating the vagal system has generated clinical interest. Existing approved vagal stimulation therapies include:
- Transcutaneous auricular VNS — stimulation of the ear’s vagal branches
- Implantable VNS devices — for epilepsy and depression
- Non-invasive abdominal VNS — under research investigation for inflammatory bowel disease
The umbilical reflex, while not itself a therapeutic target, demonstrates the same principle — that visceral afferent stimulation can effectively engage the vagal system.
FAQ: Belly Button Vagus Nerve Reflex
Q1: Can stimulating the belly button be dangerous for people with heart conditions? People with bradyarrhythmias (already slow heart rates), sick sinus syndrome, or high-degree heart block should avoid deep sustained umbilical pressure — the additional vagal slowing could produce dangerous heart rate reduction. People with vasovagal syncope history are also at higher risk of fainting from umbilical stimulation. For healthy adults, casual belly button touching is safe — the risk is primarily with sustained, deep, directed pressure toward the peritoneum.
Q2: Is there a way to stop the dizziness after touching your belly button? Yes — the most effective immediate intervention is to lie down or lower your head below your heart level (increasing cerebral blood flow despite the lower blood pressure), which typically resolves the dizziness within 30–60 seconds. Stopping the belly button stimulation removes the afferent input driving the reflex. Tensing the leg muscles while sitting (muscle contractions increase venous return and blood pressure) is also effective. Drinking water beforehand reduces the blood pressure drop magnitude by improving baseline blood volume.
Q3: Why do newborns sometimes have bradycardia when their umbilical cord is handled? Newborn umbilical cord handling shown triggering the same reflex — the umbilical cord’s vascular structures contain nerve fibers that can activate the vagal reflex during manipulation. This is one reason why pediatric caregivers learn to handle the umbilical stump gently and why umbilical cord clamping technique matters. The newborn’s vagal system is highly reactive — shown as producing more pronounced bradycardic responses to vagal stimulation than adults.
Q4: Does the belly button vagus nerve reflex change with age? Yes — vagal tone and reflex sensitivity shown changing throughout life. Children and young adults typically show stronger reflexes. The vagal reflex tends to attenuate with age — particularly in the context of the autonomic dysfunction associated with aging, cardiovascular disease, and diabetes. This is why older adults are less likely to experience dramatic vasovagal responses to belly button stimulation but more likely to experience orthostatic hypotension from the same reflex mechanism.
Q5: Can the belly button reflex be trained or habituated? Like other reflexes, repeated stimulation can produce some degree of habituation — the reflex response shown attenuating with repeated identical stimulation as the NTS shown down-regulating its response to a repeated, non-threatening stimulus. Regular practitioners of yoga and meditation — who may regularly experience abdominal pressure changes during practice — shown potentially having somewhat habituated umbilical reflexes. However, this habituation is partial and the underlying anatomical connection remains.
The belly button vagus nerve reflex is a perfect demonstration of how fetal anatomy creates adult neurological realities — the obliterated vascular structures of the umbilical cord maintaining their anatomical connections to the liver, bladder, and peritoneum, and the peritoneal visceral afferents providing functional access to the vagal system that coordinates heart rate, blood pressure, and gastrointestinal function.
In 3D, rendering the complete pathway — from peritoneal mechanoreceptor activation through spinal cord and NTS integration to SA node acetylcholine release and cardiovascular response — makes visible a connection that exists in every human body but is known to almost none of them.
Your belly button is connected to your heart. Literally. Through a nerve pathway that was established before you were born.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured vagal signal dynamics and SA node electrophysiology response |
| Material/Shader | Subsurface Scattering (SSS) | Simulating vagus nerve pathway and cardiac tissue visualization |
| Physics Engine | Volumetric Particle System + Electrostatic | Visualized acetylcholine release, GIRK channel activation, heart rate slowing |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of belly button vagus nerve reflex anatomy |
Read more on Why Does Touching Your Belly Button Make You Dizzy?
Pingback: Why Does Touching Your Belly Button Make You Dizzy? 3D Science