The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore what happens if you hold your poop — visualizing colonic water absorption mechanics, fecal hardening progression, rectal wall distension, and the systemic consequences of chronic stool retention. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: What Happens If You Hold Your Poop? (The Atomic Answer)
What happens if you hold your poop involves a progressive sequence of mechanical and physiological changes — beginning within minutes of suppressing the defecation reflex and escalating over hours and days into potentially serious complications.
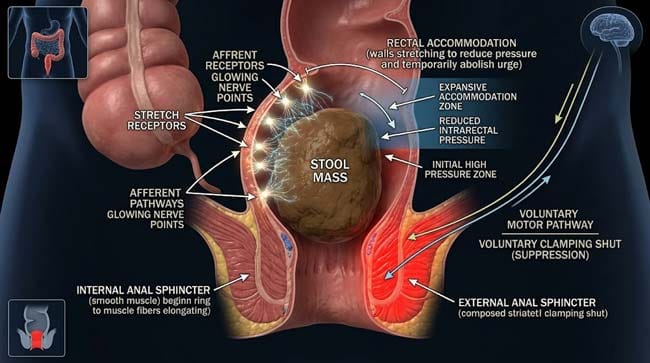
- The Immediate Response: When you suppress the urge to defecate, the external anal sphincter contracts voluntarily — shown in our 3D model as a ring of striated muscle clamping shut. The rectum shown accommodating the stool mass through receptive relaxation — its walls expanding to reduce pressure and temporarily abolishing the urge.
- The Water Problem: The large intestine absorbs water from stool continuously — at a rate of approximately 1–2 liters per day. Every hour stool remains in the colon, more water is extracted — progressively hardening the stool mass.
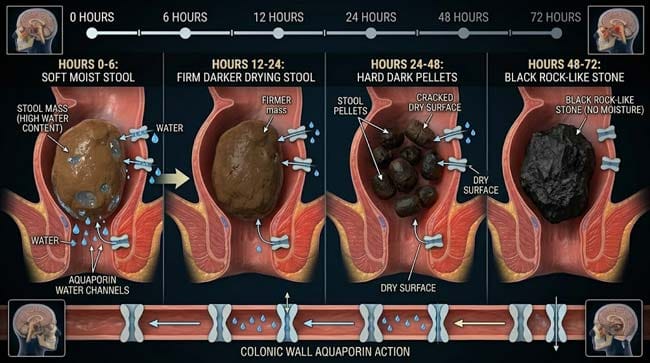
- The Hardening: Within 12–24 hours of retention, soft, easily passed stool shown progressively transforming into hard, dry pellets. Within 48–72 hours, the stool can become stone-like — requiring significant straining or medical intervention to pass.
- The Extreme Case: Chronic long-term retention produces fecaloma — a rock-hard compacted mass of desiccated feces that can grow large enough to compress adjacent organs and require surgical removal.

My 3D Discovery: Rendering the “Water Extraction Machine”
When I was building the colonic water absorption model for this simulation, the most visually striking sequence was watching the stool mass transform over a 72-hour retention period. Fresh stool entering the colon shown as a soft, moist mass — its surface shown glistening with water content, its consistency shown as easily deformable under gentle pressure.
Over 24 hours of simulated retention, the water content shown progressively decreasing — the surface shown drying, the mass shown becoming increasingly rigid. At 48 hours, shown as a noticeably harder, darker mass. At 72 hours, shown as a dense, dry, rock-like object that the colonic wall can barely move through peristalsis.
3D Observation: The most compelling visual in this simulation is the water extraction process at the cellular level. The colonic epithelium shown as a densely packed layer of columnar cells — each shown with active aquaporin water channels pumping water from the colonic lumen into the surrounding capillary network. When stool remains stationary in the colon, these aquaporins shown continuing to extract water from all exposed surfaces simultaneously — the stool mass shown shrinking and hardening from the outside inward, like a grape desiccating into a raisin.
Stage 1: The Normal Defecation Reflex — What You’re Suppressing
The Gastrocolic Reflex:
Normal bowel movements are triggered by the gastrocolic reflex — a neurological response to food entering the stomach that triggers mass peristaltic movements in the colon. In our 3D neurological model:
- Food shown entering the stomach → stretch receptors shown activating → vagal nerve signal shown traveling to the enteric nervous system → mass peristaltic contractions shown sweeping fecal material from the transverse colon through the descending colon and into the rectum
This is why the urge to defecate most commonly occurs after meals — particularly breakfast (the first meal after overnight fasting produces the strongest gastrocolic reflex).
The Defecation Reflex Sequence:
In our 3D defecation model, I rendered the complete normal sequence:
Step 1 — Rectal Filling Fecal material shown arriving in the rectum from the sigmoid colon. The rectal walls shown initially relaxing (receptive relaxation) to accommodate the incoming material without immediately triggering strong pressure signals.
Step 2 — Stretch Receptor Activation As rectal volume increases, mechanoreceptors in the rectal wall shown activating — threshold typically reached at approximately 150–300ml of rectal volume. Signals shown traveling through the pudendal nerve to the spinal cord and upward to the brain.
Step 3 — Internal Anal Sphincter Relaxation (Recto-Anal Inhibitory Reflex) The internal anal sphincter — smooth muscle, involuntary — shown automatically relaxing in response to rectal distension. This is the component you cannot consciously control.
Step 4 — Urge to Defecate The brain receives the rectal fullness signal and registers the urge to defecate. At this point, the person has a choice — proceed with defecation or voluntarily contract the external anal sphincter to suppress the reflex.
Step 5 — Voluntary Suppression The external anal sphincter — shown as striated muscle under conscious control — contracts voluntarily. Simultaneously, the rectum shown undergoing accommodation — its walls shown stretching further and the stretch receptors shown reducing their firing rate as the rectal wall adjusts to the increased volume. The urge temporarily subsides.
| Defecation Reflex Stage | Control Type | 3D Visual | Suppression Effect |
|---|---|---|---|
| Gastrocolic reflex | Involuntary | Peristaltic wave from stomach signal | Cannot be suppressed — stool still moves |
| Rectal filling | Involuntary | Stool shown entering rectum | Cannot be prevented |
| Internal sphincter relaxation | Involuntary | Smooth muscle ring opening | Cannot be consciously prevented |
| Urge perception | Conscious awareness | Brain signal shown | Can be acknowledged and suppressed |
| External sphincter contraction | Voluntary | Striated muscle clamping shut | The actual suppression mechanism |
| Rectal accommodation | Involuntary response to suppression | Rectal walls expanding further | Temporarily abolishes urge |
According to the American Gastroenterological Association, the defecation reflex — and the rectal accommodation that follows voluntary suppression — is a normal physiological process. Occasional suppression for social reasons is not harmful. Chronic, habitual suppression is associated with rectal hyposensitivity, constipation, and fecal impaction development. AGA: Constipation and Defecation Disorders
Stage 2: The Water Extraction Timeline — How Stool Becomes Stone
The Colon’s Water Absorption System:
The large intestine is a water extraction machine — designed to absorb water from intestinal contents and return it to the body. In our 3D colonic model, I rendered the water absorption mechanism:
Aquaporin Water Channels The colonic epithelium shown densely populated with aquaporin-3 and aquaporin-4 water channel proteins — shown as hourglass-shaped transmembrane proteins that allow water to pass through the cell membrane in response to osmotic gradients.
Electrolyte-Driven Absorption Sodium ions shown being actively pumped out of the colonic lumen by Na+/K+ ATPase pumps — creating an osmotic gradient that draws water through the epithelium passively. In the animation, sodium ions shown being actively transported out, water shown following osmotically.
The Absorption Rate:
- Normal daily water absorption by the colon: 1.5–2 liters
- Maximum absorption capacity: up to 5 liters per day
- Fresh stool water content: approximately 75% by weight
- Hard stool water content: approximately 50–55% by weight
The 72-Hour Hardening Progression:
In our time-lapse simulation, I tracked a stool mass retained in the sigmoid colon:
Hours 0–6: Stool shown as soft, moist mass — water content approximately 75%. Surface shown glistening. Consistency shown as easily deformable. Color shown as medium brown.
Hours 6–12: Surface drying beginning. Water content dropping to 65–70%. Mass shown slightly firmer. Movement by peristalsis shown becoming slightly more difficult.
Hours 12–24: Significant hardening. Water content 60–65%. Surface shown clearly dry and cracked. Normal peristalsis shown struggling to move the mass. Straining required for passage.
Hours 24–48: Hard, pellet-like consistency. Water content 55–60%. Mass shown dark brown, dry, fragmented into multiple hard pellets. Significant straining required.
Hours 48–72+: Stone-like consistency. Water content approaching 50%. Mass shown almost black, rock-hard. Manual disimpaction or medical intervention may be required for passage. Risk of anal fissure from forced passage is significant.
| Time | Water Content | Consistency | Passage Difficulty | Risk Level |
|---|---|---|---|---|
| 0–6 hours | ~75% | Soft, moist | Easy | None |
| 6–12 hours | 65–70% | Slightly firm | Easy to moderate | Low |
| 12–24 hours | 60–65% | Firm | Moderate — some straining | Low-Moderate |
| 24–48 hours | 55–60% | Hard, pellets | Significant straining | Moderate |
| 48–72+ hours | ~50% | Stone-like | Medical intervention may be needed | High |
Stage 3: The Complications — What Chronic Holding Causes
Rectal Hyposensitivity:
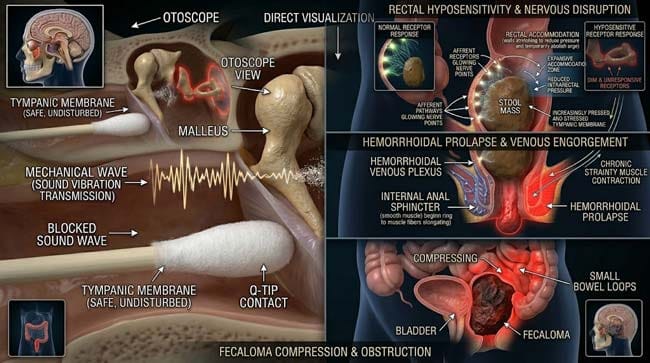
One of the most serious long-term consequences of habitual stool holding is rectal hyposensitivity — the gradual loss of rectal stretch receptor sensitivity from chronic overdistension.
In our 3D receptor model, I showed what happens when the rectum is repeatedly overdistended:
- Normal rectum: stretch receptors shown activating at approximately 150–200ml volume
- Chronically overdistended rectum: same receptors shown requiring 300–500ml+ before activating
- Severely hyposensitive rectum: receptors shown barely responding even to maximum distension — the person shown experiencing little urge to defecate even when severely constipated
This progressive desensitization shown creating a vicious cycle — the person must hold larger and larger volumes before feeling the urge, leading to longer retention periods and further receptor desensitization.
Rectal Prolapse:
Chronic straining against hardened stool shown placing extreme pressure on the rectal support structures. In our 3D structural model:
- Pelvic floor muscles shown under sustained stress from repeated Valsalva maneuvers during straining
- Puborectalis muscle shown becoming progressively overstretched
- In severe cases, the rectal mucosa shown beginning to prolapse — the inner rectal lining shown protruding through the anal canal
Hemorrhoidal Development:
The increased venous pressure from chronic straining shown causing engorgement of the hemorrhoidal venous plexus — shown as the cushions of vascular tissue in the anal canal becoming increasingly engorged and prolapsed with each straining episode.
Anal Fissure:
The passage of extremely hard stool shown causing the characteristic linear tear in the anoderm at the posterior midline — shown as a painful split in the anal canal skin that heals poorly due to the repeated trauma of subsequent bowel movements.
The Fecaloma Pathway:
In the most extreme cases of chronic retention — shown particularly in patients with neurological conditions, severe constipation disorders, or elderly individuals with reduced bowel motility — the retained stool shown progressing to fecaloma formation:
Stage 1: Stool accumulates over days to weeks in the rectum and sigmoid colon Stage 2: Continuous water extraction hardens the mass progressively Stage 3: New stool arriving from proximal colon shown being added to the growing mass Stage 4: The mass shown reaching a size where normal passage is impossible Stage 5: The fecaloma shown compressing adjacent organs — bladder, urethra, and small bowel loops
| Complication | Mechanism | Timeline | Reversibility |
|---|---|---|---|
| Rectal hyposensitivity | Chronic stretch receptor fatigue | Months to years | Partial — requires bowel retraining |
| Rectal prolapse | Chronic straining and pelvic floor weakening | Years | Surgical repair may be needed |
| Hemorrhoids | Chronic venous engorgement from straining | Months to years | Conservative to surgical treatment |
| Anal fissure | Hard stool trauma to anoderm | Single event | Usually heals; chronic fissures require treatment |
| Fecaloma | Extreme chronic retention with desiccation | Weeks to months | Medical/surgical removal required |
FAQ: What Happens If You Hold Your Poop?
Q1: How long is too long to hold your poop? Occasional suppression for 1–3 hours for social or practical reasons is normal and harmless. The concerning pattern is habitual daily suppression — particularly in children who withhold stool due to fear of pain (from previous fissures) or anxiety. Adults who consistently delay defecation for many hours daily over months develop the cycle of rectal hyposensitivity and progressive constipation. As a general guideline — if you feel the urge and a toilet is reasonably accessible, going promptly is healthier than habitual suppression.
Q2: Is it true your body can reabsorb toxins from held stool? This is a common belief — and partially true. The colon does absorb water and some small molecules from fecal material, including bacterial metabolic byproducts. However, the liver efficiently processes most reabsorbed compounds. The systemic toxicity from stool retention is not from dramatic “toxin reabsorption” but from the mechanical consequences — bloating, discomfort, reduced appetite, and the downstream complications of progressively hardened stool.
Q3: What is the correct technique for passing hard stool? Squatting position (or using a footstool to elevate feet while on a toilet) straightens the anorectal angle — shown in the 3D model as the puborectalis muscle relaxing and the rectal passage becoming more aligned with the anal canal. This position reduces the straining required significantly. Adequate hydration (1.5–2 liters of water daily) and dietary fiber (25–38g daily) maintain stool softness. Osmotic laxatives (polyethylene glycol) are safe for short-term use for already-hardened stool.
Q4: Why does holding poop sometimes make the urge disappear completely? This is the rectal accommodation mechanism — the rectal walls shown relaxing and the stretch receptors shown reducing their firing rate after the rectum adjusts to increased volume. The urge disappears not because the stool has gone anywhere but because the rectum has accommodated it. The stool remains, continuing to desiccate, until the gastrocolic reflex of the next meal or mass peristalsis re-triggers the defecation urge.
Q5: Can children permanently damage their bowels from stool withholding? Yes — childhood stool withholding is a significant pediatric gastroenterology concern. Children who withhold stool due to pain or anxiety develop rectal hyposensitivity and megarectum (chronically dilated rectum) that can take months to years of treatment to resolve. The condition is called functional non-retentive fecal incontinence in its advanced form — where the chronically dilated rectum loses its ability to sense fullness and the child experiences involuntary soiling. Early intervention with laxative therapy and behavioral support is critical.
Conclusion: The Raisin Effect — Why Timing Matters
The colon is an extraordinarily efficient water extraction system — and it does not pause its work while you wait for a more convenient moment. Every hour of stool retention is an hour of water extraction, progressive hardening, and increasing difficulty of passage.
In 3D, watching the stool mass transform from soft and easily passed to stone-like over 72 hours — and watching the colonic epithelium’s aquaporin channels pumping water continuously regardless of what the person is doing — makes the urgency of the defecation reflex physiologically understandable.
The urge exists for a reason. The timing it suggests is usually correct. And the consequences of consistently overriding it compound quietly over time — in receptors that stop working, in walls that stop feeling, and in masses that stop moving.
Let it go.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured colonic water absorption dynamics and stool hardening progression |
| Material/Shader | Subsurface Scattering (SSS) | Simulating colonic tissue and progressive stool desiccation |
| Physics Engine | Fluid Dynamics + Soft Body | Visualized aquaporin water transport, stool consistency changes, peristaltic mechanics |
| Goal | Educational / Science Visualization | Research-referenced 3D breakdown of stool retention physiology |
Read more on Fecaloma: The 3D Science of What Happens When Poop Turns to Stone
Pingback: Fecaloma: What Is It?The 3D Science of Poop Turning to Stone