The Creator’s Note & Disclaimer: As a 3D artist at WhatIfBody3D, I rendered this scenario at 120 FPS. Our models explore how to remove an insect from the ear safely — visualizing why amateur removal attempts fail, oil immobilization mechanics, irrigation physics, and the professional extraction protocol that protects the tympanic membrane. This visualization is part of our “What If” series and is for educational and informational purposes only, as stated in our About Page.
Quick Answer: How to Remove Insect From Ear? (The Atomic Answer)
How to remove insect from ear safely? The answer begins with what NOT to do — because the most instinctive responses make the situation dramatically worse.
- Never use tweezers or fingers: A live insect responds to any contact by pressing harder against the eardrum, biting, and scratching — causing more pain and risk of tympanic membrane damage than doing nothing.
- The First Step is Always Immobilization: Before any removal attempt, the insect must be killed or immobilized using mineral oil, olive oil, or baby oil poured into the ear canal — blocking the insect’s spiracles (breathing pores) within 1–2 minutes.
- The Second Step is Irrigation: Once immobilized, warm water irrigation flushes the canal effectively in most cases — no instruments required.
- When to Go to the ER: If oil and irrigation do not resolve the situation within 10–15 minutes, professional removal with otoscope guidance and specialized instruments is required — particularly if the insect is large or deeply lodged.

My 3D Discovery: Rendering the “Wrong Way” vs “Right Way”
When I was building the removal mechanics model for this simulation, I decided to render both the incorrect amateur approach and the correct professional approach side by side — to make the mechanical reasons for each recommendation visually obvious.
In the “wrong way” simulation, tweezers shown entering the ear canal. The moment the metal contacts the cockroach body — shown as the insect’s sensory hairs detecting vibration — the cockroach’s defensive response activates instantly. Its legs shown pressing harder against the tympanic membrane. Its mandibles shown opening. The additional contact shown producing more pain signals along the auriculotemporal nerve. The tweezer tips shown with high risk of canal wall laceration.
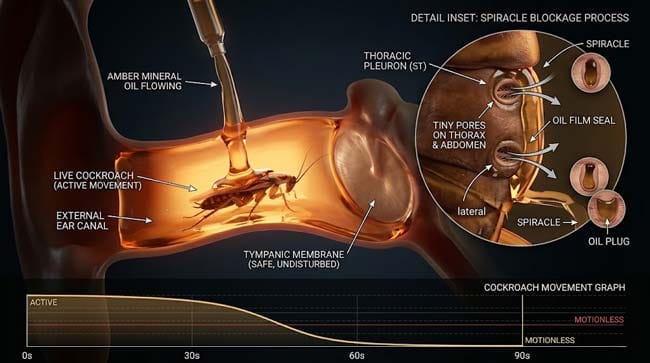
In the “right way” simulation, oil shown flowing into the canal and surrounding the insect from all sides. Within 90 seconds, the insect’s spiracles — shown as tiny pores along its thorax — blocked by the oil film. Oxygen access cut off. The insect shown progressively slowing, then becoming motionless. The canal shown calm. The subsequent irrigation shown easily flushing the immobilized body outward.
3D Observation: The contrast between the two approaches is immediately obvious in the animation. The amateur tweezer attempt shown producing a cascade of escalating responses — more movement, more membrane contact, more pain signals. The oil immobilization shown producing a progressive calming — the insect’s activity graph shown declining steadily over 90 seconds until complete stillness. Same starting situation. Completely opposite trajectories depending on the first decision made.
Stage 1: Why Most Instinctive Removal Attempts Fail
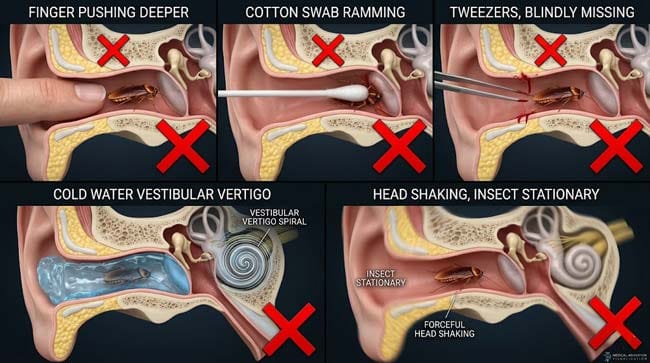
The Five Most Common Wrong Approaches — And Why Each Makes It Worse:
Wrong Approach 1 — Using Fingers
The instinctive first response: reach into the ear with a finger to push the insect out. In our 3D simulation:
- Human finger diameter: approximately 18–20mm
- Ear canal diameter: 6–8mm
The finger cannot enter the canal. What it does instead:
- Compresses the insect against the canal wall — triggering defensive response
- Pushes the insect deeper into the canal
- Presses any leg fragments further toward the eardrum
In the animation, finger contact shown immediately pushing the cockroach forward — the insect’s legs shown pressing directly against the tympanic membrane under the added pressure.
Wrong Approach 2 — Using Cotton Swabs
Cotton swabs are the most dangerous amateur tool for this situation. In our 3D mechanical model:
- Cotton swab diameter: approximately 6mm — similar to canal diameter
- Effect: acts as a ram — pushing the insect directly against the eardrum
- Risk: the cotton tip shown compressing against the insect and eardrum simultaneously
In the animation, cotton swab insertion shown pushing the cockroach progressively deeper — the eardrum shown deflecting inward under combined swab and insect pressure.
Wrong Approach 3 — Using Tweezers
Tweezers appear logical — grab the insect and pull it out. In our 3D procedure simulation:
- The ear canal’s S-curve prevents direct visual line to the insect
- Tweezers inserted blind shown consistently contacting canal walls rather than the insect
- Any contact with a live cockroach shown triggering immediate defensive response
- Tweezer tips shown with high laceration risk on the thin inner canal skin
Additionally: cockroach mandibles can bite tweezer-wielding fingers through the canal — shown in the simulation as the cockroach attempting to bite any object making contact.
Wrong Approach 4 — Attempting to Flush With Cold Water
Cold water in the ear canal produces two problems shown in our simulation:
- Caloric vestibular response: Cold water shown contacting the tympanic membrane and triggering the vestibular system — producing immediate severe vertigo, nausea, and vomiting
- Insect agitation: Cold water shown agitating the live insect rather than flushing it — the cockroach shown moving more frantically in response to the temperature change
Warm water is required for irrigation — cold water causes more harm than good.
Wrong Approach 5 — Vigorous Head Shaking
Shown in the animation as entirely ineffective — the canal’s S-curve prevents gravity from removing an insect that has moved past the cartilaginous section. Head shaking shown producing no displacement of the insect while causing significant vestibular disturbance and pain from the insect’s reactive movement.
| Wrong Approach | Intended Effect | Actual Effect | Risk Level |
|---|---|---|---|
| Fingers | Push insect out | Pushes insect deeper, triggers defense | Moderate |
| Cotton swabs | Scoop insect out | Rams insect against eardrum | High |
| Tweezers (blind) | Grab and extract | Canal lacerations, insect agitation | Very High |
| Cold water flush | Flush insect out | Severe vertigo, insect agitation | High |
| Head shaking | Gravity removal | No effect, pain amplification | Low-Moderate |
According to the American Academy of Otolaryngology-Head and Neck Surgery, amateur removal attempts for ear canal foreign bodies — particularly live insects — are associated with significantly higher rates of complications including tympanic membrane perforation, canal laceration, and insect fragmentation (leaving parts in the canal) compared to professional extraction. AAO-HNS: Ear Foreign Body Management
Stage 2: The Correct Protocol — Step by Step
The Oil Immobilization Method — The Critical First Step
The single most important action anyone can take before seeking medical care is oil immobilization. This is safe, effective, available in most households, and dramatically improves outcomes compared to any other first response.
How Oil Immobilization Works:
Insects breathe through spiracles — small openings along the thorax and abdomen that connect to the tracheal system. In our 3D insect respiratory model, I rendered these spiracles as tiny valve-like pores distributed along the cockroach’s body surface.
When oil is poured into the ear canal, it flows around the insect’s body — shown in the simulation as the oil filling all available space in the canal. The oil creates a film over the spiracle openings, blocking air exchange. Without oxygen, the cockroach becomes progressively incapacitated:
- 0–30 seconds: Increased movement as insect attempts to escape
- 30–90 seconds: Movement slowing as oxygen deprivation begins
- 90–120 seconds: Near-complete immobilization
- 2–3 minutes: Full immobilization
What to Use:
- Mineral oil ✅ — most effective, readily available
- Olive oil ✅ — equally effective, available in most kitchens
- Baby oil ✅ — effective alternative
- Vegetable oil ✅ — works but slightly less viscous
- Water ❌ — does not block spiracles, cockroach remains active
- Alcohol ❌ — may cause burning pain, can damage canal tissue
How to Administer:
In our 3D procedure simulation, I showed the correct oil administration technique:
- Tilt head with affected ear facing upward
- Gently pull ear pinna backward and upward to straighten canal
- Pour 3–5ml of oil into the canal entrance
- Allow oil to flow inward — do not use a dropper if syringe unavailable
- Maintain head position for 2–3 minutes until insect is immobilized
- Keep head tilted to prevent oil from draining
The Warm Water Irrigation — Step Two
Once the insect is immobilized, warm water irrigation is the most effective non-instrumental removal method. In our 3D irrigation simulation:
Equipment:
- Bulb syringe or irrigation syringe (available at pharmacies)
- Water at body temperature (37°C/98.6°F) — critical that it is warm, not cold
Technique:
- Tilt head with affected ear downward over a basin
- Gently direct warm water stream along the upper canal wall — not directly at the eardrum
- Water shown flowing around and behind the immobilized insect
- Hydraulic pressure shown pushing the insect outward
- Multiple gentle irrigations typically needed for complete removal
Why Directing Water Along the Upper Wall:
In the 3D fluid dynamics model, I showed why directing water at the eardrum directly is problematic — it creates a pressure wave that can be painful and produce a caloric response. Directing water along the canal wall instead creates a flowing hydraulic current that carries the insect out without direct membrane pressure.
| Irrigation Variable | Correct | Incorrect | Effect of Error |
|---|---|---|---|
| Water temperature | 37°C (body temp) | Cold or very hot | Cold → severe vertigo; hot → burns |
| Water direction | Along upper canal wall | Directly at eardrum | Direct pressure → pain, membrane risk |
| Pressure | Gentle, controlled | Forceful | Forceful → barotrauma risk |
| Head position | Affected ear down | Affected ear up | Water retention, ineffective drainage |
Stage 3: Professional Removal — What Happens at the ER
When Home Methods Are Insufficient:
Professional removal is required when:
- Oil and irrigation do not remove the insect after 2–3 attempts
- The insect is large (too large for irrigation to flush)
- Significant pain, bleeding, or hearing loss is present
- The insect has fragmented (parts remaining in canal)
- Tympanic membrane perforation is suspected
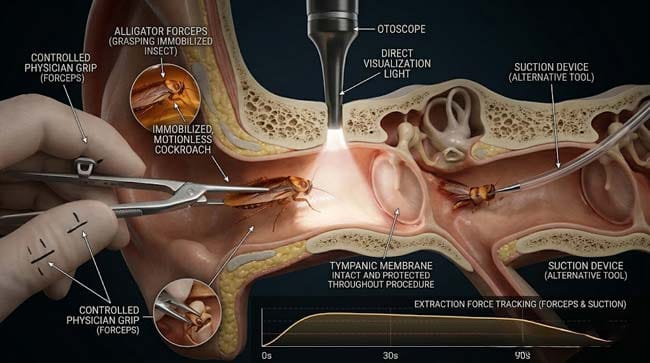
The Emergency Room Protocol:
In our 3D ER procedure simulation, I rendered the complete professional removal sequence:
Step 1 — Otoscopic Examination The physician shown using an otoscope to directly visualize the canal — confirming insect presence, location, size, and whether the tympanic membrane is intact.
Step 2 — Anesthetic Immobilization If the insect remains active, 2% lidocaine solution shown being instilled — immobilizing the insect through direct nervous system effect while simultaneously providing local anesthesia to the canal tissue.
Step 3 — Instrumented Extraction
Depending on the situation, several instruments shown in use:
Alligator forceps — shown grasping the immobilized insect body under direct otoscope visualization. The key shown: grasping the insect’s central body mass, not legs (which detach easily), and extracting with a single smooth motion.
Suction devices — shown creating negative pressure that draws the insect outward without mechanical grasping — preferred for fragile insects that might fragment with forceps.
Right-angle hooks — shown being used to dislodge insects pressed against the eardrum, gently separating the insect from the membrane before extraction.
Step 4 — Fragment Check After apparent removal, the physician shown performing careful otoscopic inspection for:
- Remaining insect legs (cockroach legs detach easily)
- Antenna fragments
- Cerumen pushed deeper by the insect
Any remaining fragments shown being removed with micro-forceps or suction before the procedure is considered complete.
Step 5 — Membrane Assessment Final otoscopic examination shown checking the tympanic membrane for:
- Integrity — no perforations
- Injection — redness indicating inflammation
- Hemotympanum — blood in the middle ear space (rare, indicates significant trauma)
| ER Removal Tool | Best Use | Mechanism | 3D Visualization |
|---|---|---|---|
| Alligator forceps | Solid, graspable insect body | Mechanical grasping under direct vision | Forceps shown under otoscope guidance |
| Suction device | Friable or fragmented insect | Negative pressure extraction | Suction cup shown drawing insect outward |
| Right-angle hook | Insect wedged against eardrum | Separation and leverage | Hook shown between insect and membrane |
| Irrigation (professional) | Post-immobilization flush | Hydraulic flow | Controlled warm water stream |
According to the American College of Emergency Physicians (ACEP), professional ear foreign body removal with proper immobilization and instrumented extraction under direct visualization has a success rate exceeding 95% with minimal complications — compared to significantly lower success rates and higher complication rates for unguided amateur attempts. ACEP: Ear Foreign Body Removal Guidelines
FAQ: How to Remove Insect From Ear
Q1: How do I know if the insect has been successfully removed? Complete removal is indicated by: cessation of the scratching or movement sounds, resolution of the intense pain, return of normal hearing sensation, and absence of the feeling of a foreign body in the ear. However, subjective improvement alone is not sufficient confirmation — medical evaluation with otoscopy is the only way to confirm complete removal and assess tympanic membrane integrity.
Q2: What if the insect dies inside the ear without being removed? A dead insect in the ear canal will not cause immediate serious harm, but it will decompose — causing increasing discomfort, discharge, and potential secondary infection from bacterial decomposition. Dead insects do not exit the canal on their own. Medical removal remains necessary regardless of whether the insect is alive or dead.
Q3: Can a cockroach lay eggs in your ear? This fear is common but essentially impossible in practice. A cockroach in the ear canal cannot access the food, water, and temperature conditions necessary for ootheca (egg case) production and incubation. The ear canal’s hostile environment — oil, cerumen, immune responses — would prevent any egg development even in the theoretical case that an egg case was deposited. Documented cases of insect egg development in the ear canal are essentially nonexistent in clinical literature.
Q4: Should I use hydrogen peroxide to remove an ear insect? No. Hydrogen peroxide is not effective for insect immobilization — it does not block spiracles the way oil does. It can cause bubbling and fizzing that increases discomfort and may agitate a live insect. It is also potentially irritating to the delicate inner canal skin. Oil is always preferable to hydrogen peroxide for this specific situation.
Q5: How long can a cockroach survive inside an ear canal? Without oil immobilization, a cockroach can survive in the ear canal for several hours — fed by the warm temperature and protected from desiccation by the humid environment. Some case reports describe insects surviving overnight before medical care was sought. This is why prompt oil immobilization and medical care are important — the longer the insect remains active, the more discomfort is experienced and the greater the cumulative risk of tympanic membrane trauma.
Conclusion: The Right Tool for the Right Situation
Removing an insect from the ear is one of the few medical situations where doing less initially is dramatically more effective than doing more. The instinct to act immediately — to grab tweezers, to insert fingers, to shake the head — is almost always counterproductive. The correct first step is to pour oil and wait.
In 3D, watching the oil flow around the cockroach’s body and seal its spiracles — and watching the insect’s movement progressively slow and stop — makes the elegance of this simple intervention immediately clear. No tools required. No pain. No risk of tympanic membrane damage. Just a 90-second immobilization that transforms a distressing emergency into a manageable medical situation.
The ear canal’s anatomy creates the trap. The oil removes the insect’s ability to make the trap worse. And professional extraction removes whatever remains.
Oil first. Always.
Further Study & External Research
3D Simulation Specs & Observations
| 3D Component | Technical Visual Setting | Observation from Viewport |
|---|---|---|
| Framerate | 120 FPS High-Speed | Captured oil immobilization dynamics and irrigation fluid mechanics |
| Material/Shader | Subsurface Scattering (SSS) + Fluid Simulation | Simulating oil viscosity, water flow, and ear canal tissue |
| Physics Engine | Fluid Dynamics + Soft Body | Visualized oil filling canal space, irrigation hydraulics, forceps mechanics |
| Goal | Educational / Science Visualization | Research-referenced 3D guide to safe insect ear removal protocol |
Read more on What Happens If a Cockroach Crawls Into Your Ear?
Pingback: What Happens If a Cockroach Crawls in Your Ear? 3D Guide